👉 Register for Free. How to Diagnose Sleep Apnea Faster in Primary Care – FREE Webinar by Dr. Audrey Wells. – Friday, April 24 at 12 PM ET

Is This Perimenopause or Insomnia? How to Tell the Difference
Is this perimenopause or insomnia? The two conditions share many symptoms and frequently occur together, making them genuinely difficult to separate. Understanding whether your sleep disruption is driven by hormonal change, a behavioral sleep disorder is essential for getting the right support.
This article reflects the clinical expertise of Dr. Avinesh Bhar, Board Certified Sleep Physician at Sliiip.com, who works with women navigating the intersection of hormonal transition and sleep medicine every day.
You cannot sleep through the night anymore. Some nights you wake up drenched. Other nights you just lie there, mind running at full speed with no obvious reason. You fall asleep fine but wake at 3 a.m. and cannot get back.
You are asking yourself: is this perimenopause or insomnia?
The honest answer is that it may be both. It may also be neither. There is a third possibility that most providers never raise, and it changes everything.
SLIIIP’s board-certified sleep physicians can do sleep evaluations for sleep apnea. Virtual consultations in all 50 states. Home sleep tests shipped to your door.
Myth vs. Reality: Perimenopause and Insomnia
Myth: If you are a woman in your 40s or 50s who cannot sleep, it is perimenopause. Hormone management will resolve it.
Reality: Perimenopause is a genuine contributor to sleep disruption, but it is frequently not the only contributor. Many women receive hormone therapy and continue to sleep poorly because a co-occurring sleep disorder, most often sleep-disordered breathing, has never been evaluated or treated.
Myth: Insomnia means you cannot fall asleep. If you fall asleep fine but wake during the night, that is something else.
Reality: Insomnia includes difficulty staying asleep and early morning waking, not just difficulty initiating sleep. Many women with perimenopause-related or primary insomnia have no trouble falling asleep initially but experience frequent, prolonged nighttime wakefulness that feels entirely outside their control.
What Is Actually Happening During Perimenopause
Perimenopause is the hormonal transition that precedes menopause, typically beginning in the early to mid-40s and lasting anywhere from two to twelve years. During this period, estrogen and progesterone levels fluctuate erratically before ultimately declining.
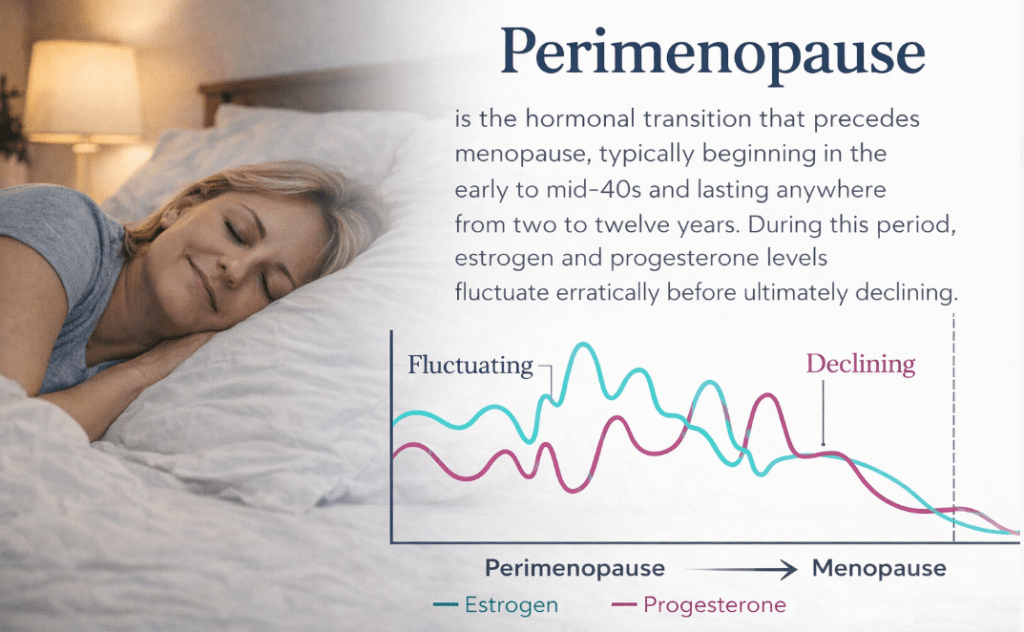
These fluctuations have direct neurological consequences for sleep. Estrogen supports serotonin activity and body temperature regulation, both critical for sleep continuity. Progesterone is converted to allopregnanolone, a neurosteroid that acts on GABA receptors to produce a calming sedative effect. As both hormones decline and fluctuate, the neurological conditions that support deep, continuous sleep become unstable.
The result is the pattern that millions of perimenopausal women recognize immediately: waking during the night, sometimes with a hot flash, sometimes with racing thoughts, sometimes for no reason that is identifiable at all.
What Is Primary Insomnia and How Is It Different
Primary insomnia, or what is now clinically classified as chronic insomnia disorder, is a condition where difficulty falling or staying asleep occurs at least three nights per week for three months or more and causes meaningful daytime impairment. It is driven by a state of hyperarousal, where the brain remains too activated for the transition into deep sleep to complete properly.
The hyperarousal driving insomnia can be physiological or psychological. Anxiety, chronic stress, conditioned wakefulness at the bed, and anticipatory worry about sleep all fuel the cycle. Once insomnia is established, it tends to self-perpetuate regardless of its original trigger.
3 Important Facts About Sleep Apnea During Perimenopause
Hormonal changes during perimenopause can significantly affect sleep quality. One of the most overlooked issues during this transition is sleep apnea, which often goes undiagnosed because its symptoms overlap with common perimenopausal complaints.
1. Hormone Decline Weakens Airway Stability
Estrogen and progesterone help maintain upper airway muscle tone during sleep. As these hormones decline during perimenopause and menopause, the muscles that keep the airway open become less effective.
This means women who never had breathing problems during their reproductive years can suddenly develop clinically significant sleep apnea during the perimenopausal transition.
2. Sleep Apnea Risk Increases After Menopause
Research shows that postmenopausal women have two to three times the prevalence of obstructive sleep apnea compared to premenopausal women with similar body composition.
The timing is important: sleep apnea symptoms often appear exactly when perimenopausal sleep problems begin, making it easy to attribute the symptoms solely to hormonal changes or insomnia.
3. Sleep Apnea in Women Often Looks Different
In perimenopausal women, sleep apnea rarely presents with the classic symptoms like loud snoring or obvious breathing pauses.
Instead, women more commonly experience:
- Fragmented sleep
- Frequent nighttime awakenings
- Morning headaches
- Brain fog and cognitive difficulty
- Mood changes
- Persistent exhaustion
These symptoms are almost identical to perimenopause-related sleep disruption, which is why sleep apnea is frequently overlooked.
How to Tell Perimenopause Sleep Disruption from Insomnia
The clinical distinction matters because the approaches differ.
Perimenopause-related sleep disruption tends to correlate with other hormonal symptoms: irregular periods, vasomotor symptoms like hot flashes and night sweats, vaginal dryness, and mood shifts that arrived around the same time as the sleep changes. The sleep problems wax and wane with hormonal fluctuation.
Insomnia tends to involve a persistent pattern of hyperarousal at the bed. The mind becomes alert and active at the moment of intended sleep or immediately after waking during the night. There is often rumination, clock-watching, or a sense of dread about whether sleep will return. The pattern is consistent rather than fluctuating.
Expert Q&A
Q: I am 47, in perimenopause, and I have been waking at 3 a.m. nearly every night for two years. My gynecologist adjusted my hormones but nothing has fully resolved. What should I be looking for?
Two years of waking at 3 a.m. despite hormonal management is a pattern that tells me we are not dealing with perimenopause alone. When a patient’s hormonal approach has been optimized and the sleep disruption continues at that frequency and consistency, I look first for sleep-disordered breathing. Perimenopause reduces upper airway muscle tone protection in ways that make sleep apnea newly emergent or significantly worse during this transition. It presents with nighttime waking and morning fatigue rather than snoring in most women. A home sleep evaluation is the step that is almost universally missing in cases like this one.
Dr. Avinesh Bhar Board Certified Sleep Physician Sliiip.com
SLIIIP’s board-certified sleep physicians can do sleep evaluations for sleep apnea. Virtual consultations in all 50 states. Home sleep tests shipped to your door.
What Helps When Perimenopause and Insomnia Overlap
- Consistent sleep and wake timing is the single most evidence-backed behavioral intervention for insomnia regardless of its origin. Going to bed and waking at the same time every day, including weekends, stabilizes the circadian rhythm and rebuilds homeostatic sleep pressure that deepens sleep quality over time.
- Cooler sleep environment. Estrogen decline disrupts thermoregulation. A room temperature of 65 to 68 degrees Fahrenheit supports the core temperature drop necessary for deep sleep initiation and reduces the frequency of vasomotor-triggered awakenings.
- Reducing pre-sleep cognitive arousal. A wind-down buffer of 45 to 60 minutes before bed, away from screens, email, and work, reduces the sympathetic activation that feeds the hyperarousal component of insomnia. Journaling, light stretching, and slow breathing are among the most accessible tools.
- Limiting alcohol. Alcohol suppresses progesterone activity and disrupts REM sleep. In perimenopausal women, alcohol worsens both the hormonal and insomnia components of sleep disruption. Even moderate evening drinking is a clinically relevant variable.
- Addressing the hyperarousal pattern directly. Cognitive behavioral therapy for insomnia is the most evidence-supported intervention for the chronic hyperarousal component of insomnia disorder. It is more effective long-term than sleep medications and addresses the conditioned wakefulness that sustains insomnia after its hormonal trigger has been managed.
When a Sleep Evaluation Changes Everything
If you have addressed your hormonal symptoms, worked on sleep hygiene, and are still waking during the night consistently, the missing diagnostic step is a sleep breathing evaluation.

A home sleep test identifies whether breathing disruptions are compounding your hormonal or insomnia-related sleep disruption. It is completed in your own bed overnight. No clinic visit required. A board-certified sleep physician reviews the results. Learn how home sleep apnea testing works at Sliiip.com.

Stop Guessing and Start Getting Answers
Is perimenopause, insomnia, or an undetected sleep disorder controlling your nights?
Sliiip.com has completed over 10,000 consultations with patients across all 50 states. No referral is needed. Home sleep testing ships directly to your door and is covered by most major insurance plans including Medicare and Tricare.
Frequently Asked Questions
Is this perimenopause or insomnia if I wake up in the middle of the night?
It may be either or both. Perimenopause-related waking is often associated with hot flashes or night sweats, while insomnia-related waking involves cognitive activation and difficulty returning to sleep. Frequently the two coexist, and a third possibility, sleep-disordered breathing, is often the unaddressed driver when both have been treated without full resolution.
What does perimenopause insomnia feel like?
Perimenopause insomnia often involves waking between 2 and 4 a.m. with racing thoughts, an inability to return to sleep, daytime fatigue, emotional sensitivity, and brain fog. It may occur alongside hot flashes and night sweats or independently. The pattern is distinct from ordinary tiredness and persists regardless of total hours spent in bed.
At what age does perimenopause insomnia start?
Perimenopausal sleep disruption most commonly begins in the early to mid-40s, though it can start earlier or later. The intensity often increases as estrogen and progesterone levels decline more steeply in the years immediately preceding menopause. Any persistent sleep change during this decade warrants clinical evaluation.
Can perimenopause cause insomnia that lasts years?
Yes. Perimenopausal hormonal disruption can initiate an insomnia cycle that becomes self-sustaining through conditioned hyperarousal. Once insomnia is established neurologically, it may persist even after hormonal management improves, because the brain has learned to remain hyperaroused in the sleep environment independently.
Does estrogen therapy help with perimenopause insomnia?
Estrogen therapy can reduce vasomotor symptoms that disrupt sleep and may improve sleep continuity for some women. However, it does not address the hyperarousal component of established insomnia, nor does it correct sleep-disordered breathing that may have emerged with the loss of hormonal airway tone protection. Additional interventions are often needed alongside hormonal management.
What is the 3 a.m. wake-up in perimenopause?
Waking at 3 to 4 a.m. during perimenopause is driven by a combination of cortisol elevation, reactive blood sugar changes, and the conditioned arousal that develops when this pattern repeats. The body anticipates waking at this time and begins the arousal process before any external trigger. This pattern requires targeted sleep medicine intervention, not simply more time in bed.
Can sleep apnea look like perimenopause insomnia?
Yes, and this is one of the most clinically consequential overlaps in women’s sleep medicine. Sleep apnea in women typically presents with nighttime waking, morning exhaustion, cognitive fog, and mood changes rather than loud snoring. These symptoms are identical to perimenopause-related sleep disruption and are routinely attributed to hormones without a breathing evaluation ever being completed.
How do I know if I have insomnia versus perimenopause sleep problems?
Insomnia involves a consistent pattern of hyperarousal at the sleep environment, where the mind becomes alert and active specifically at the time of intended sleep. Perimenopausal disruption tends to correlate with other hormonal symptoms and fluctuate over time. In practice, both mechanisms frequently operate simultaneously, and a clinical evaluation is more useful than self-classification alone.
Is it safe to take sleep medications for perimenopause insomnia?
Sleep medications may provide short-term relief but do not address the underlying hormonal, psychological, or structural causes of perimenopausal insomnia. They also suppress breathing in ways that can worsen undiagnosed sleep apnea. A clinical evaluation before initiating sleep medications is the appropriate and safer sequence.
What tests help differentiate perimenopause from insomnia?
Hormonal panels including FSH, estradiol, and progesterone can confirm perimenopausal status. A clinical sleep evaluation or overnight home sleep test assesses sleep-disordered breathing. Cognitive behavioral assessment by a sleep-trained clinician can evaluate the hyperarousal component. All three perspectives together provide the most complete picture.
Can perimenopause cause anxiety that makes insomnia worse?
Yes. Estrogen supports serotonin activity, and its decline during perimenopause can increase baseline anxiety and emotional reactivity. This hormonal anxiety directly feeds the hyperarousal mechanism of insomnia, creating a compounding cycle where hormonal change worsens insomnia, and insomnia elevates cortisol which worsens anxiety.
What is the most effective treatment for perimenopause insomnia?
The most effective approach addresses each contributing factor directly. Hormonal management for vasomotor and neurological hormonal contributions. Cognitive behavioral therapy for insomnia for established hyperarousal. Sleep breathing evaluation to rule out or treat sleep apnea. These interventions are most effective when pursued in coordination with a board-certified sleep physician.
Latest posts
-
Is My Sleep Pattern Normal? What a Normal Sleep Pattern Looks Like
If you have ever lain awake wondering whether your nights match everyone else’s, learning what a normal sleep pattern looks like can bring real peace of mind, says Dr. Avinesh…
-
Spike in Cortisol: How Workplace Stress Destroys Men’s Sleep Cycles
After a long, high pressure day at work, a spike in cortisol can follow men straight into the bedroom and quietly wreck a good night of rest, says Dr. Avinesh…
-
Overthinking at Night
Overthinking at night can turn the quietest hours into the loudest part of the day, and Dr. Avinesh Bhar, Board-Certified Sleep Physician at SLIIIP.com, hears this complaint more than almost…
Get updates
Spam-free subscription, we guarantee. This is just a friendly ping when new content is out.

