👉 Register for Free. Why Am I So Tired? The Hidden Women’s Health Issues Behind Fatigue, Hormones, and Sleep – Upcoming Webinar on Friday, March 13th, 11:00 AM ET with Dr. Audrey Wells.


Hormonal Insomnia: Why Your Hormones Are Destroying Your Sleep
Hormonal insomnia refers to sleep disruption driven by fluctuations in estrogen, progesterone, cortisol, and other hormones. It affects millions of women during perimenopause, menopause, pregnancy, and the postpartum period. Hormonal insomnia is systematically underdiagnosed because its connection to both hormonal change and underlying sleep disorders is rarely explored together.
This article reflects the clinical expertise of Dr. Avinesh Bhar, Board Certified Sleep Physician at Sliiip.com, who has guided thousands of patients through the intersection of hormonal change and sleep-disordered breathing that conventional medicine too often addresses separately.
SLIIIP’s board-certified sleep physicians can do sleep evaluations for sleep apnea. Virtual consultations in all 50 states. Home sleep tests shipped to your door.
Research from the National Sleep Foundation reports that women are 40 percent more likely than men to experience insomnia symptoms throughout their lives, with hormonal transitions identified as a primary contributing factor.
Myth vs. Reality: Hormonal Insomnia
Myth: Trouble sleeping during menopause is just hot flashes. Manage the hot flashes and the sleep will follow.
Reality: Hormonal insomnia involves multiple mechanisms beyond temperature dysregulation. Estrogen and progesterone have direct neurological effects on sleep architecture, and their decline affects the depth, continuity, and restorative quality of sleep independent of night sweats or hot flashes.
Myth: Hormonal insomnia is essentially an anxiety problem and responds primarily to cognitive or psychological support.
Reality: While hormonal insomnia is often accompanied by anxiety, the root cause is physiological. Hormonal shifts alter neurotransmitter activity, circadian timing, and upper airway muscle tone in ways that create genuine sleep disruption regardless of psychological state or stress management.
What Is Hormonal Insomnia?
Hormonal insomnia is a pattern of sleep disruption directly tied to hormonal fluctuation rather than primarily behavioral or environmental causes. It encompasses difficulty falling asleep, frequent nighttime awakenings, early morning waking, and non-restorative sleep that worsens at predictable points in hormonal cycles.
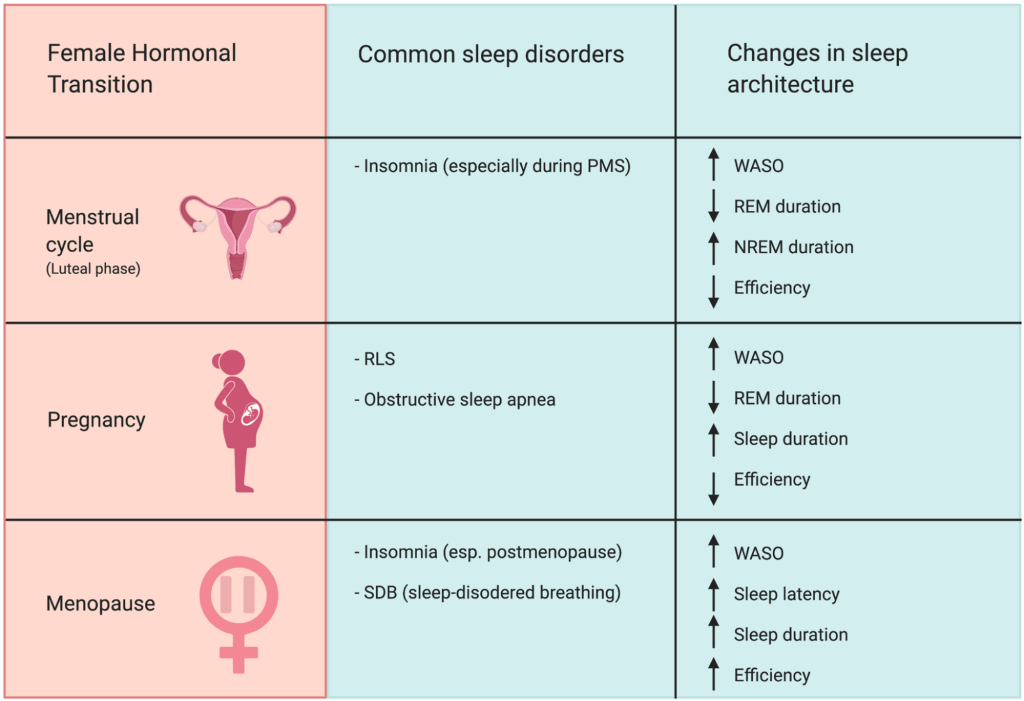
It is most prevalent during perimenopause and menopause but also affects women during the luteal phase of the menstrual cycle, during pregnancy, and in the postpartum period. The condition sits at a clinical crossroads between sleep medicine and endocrinology.
According to the U.S. Department of Health and Human Services Office on Women’s Health, insomnia is more common in women than men and hormonal changes are a key driver across the lifespan.
Hormonal insomnia is frequently undertreated because providers address either the hormonal aspect or the sleep aspect without connecting the two. Women fall through this gap for years.
Which Hormones Disrupt Sleep?
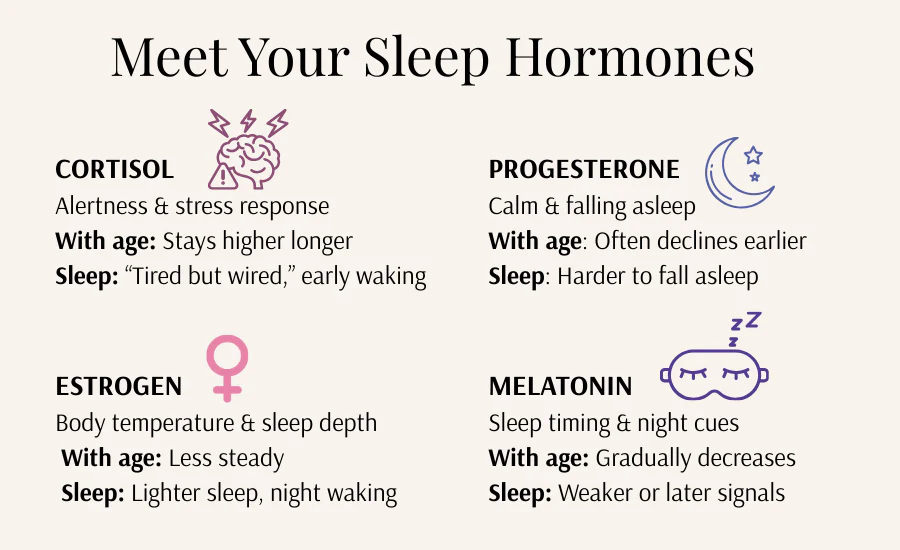
Estrogen has significant regulatory influence on sleep architecture. It supports serotonin production and promotes sleep continuity throughout the night. As estrogen levels decline during perimenopause and menopause, slow-wave sleep decreases, REM sleep fragments, and nighttime arousal increases in frequency.
Progesterone has sedative properties through its conversion to allopregnanolone, which acts on GABA receptors in the brain. When progesterone drops sharply, as it does before menstruation and during early perimenopause, the calming neurological effect it provided diminishes. The result is heightened nighttime arousal and an inability to stay asleep.
Cortisol regulates the timing of waking and alertness through a daily rhythm that peaks in the morning and declines toward evening. Chronic stress, sleep deprivation, and metabolic disruption flatten this curve. Elevated evening cortisol delays sleep onset and promotes early morning waking at 3 to 5 a.m.
Thyroid hormones affect metabolic rate and body temperature, both of which influence sleep quality. Subclinical thyroid dysfunction is an underrecognized contributor to hormonal insomnia, particularly in women over 40. The National Library of Medicine has detailed background on thyroid conditions and their systemic effects.
SLIIIP’s board-certified sleep physicians can do sleep evaluations for sleep apnea. Virtual consultations in all 50 states. Home sleep tests shipped to your door.
Hormonal Insomnia During Perimenopause and Menopause
Perimenopause typically begins in the mid-to-late 40s and may last four to eight years before menopause. During this transition, estrogen and progesterone fluctuate erratically before declining. These fluctuations directly disrupt sleep architecture in ways that feel unpredictable and uncontrollable.
Women in perimenopause commonly report taking longer to fall asleep, waking multiple times during the night, and rising earlier than intended. Night sweats compound these disruptions by raising core body temperature at precisely the time the body needs to cool for deep sleep initiation.
After menopause, the sustained decline in estrogen and progesterone produces a more stable but chronically lower hormonal baseline. Sleep architecture shifts permanently, with reductions in deep slow-wave sleep that affect both physical recovery and cognitive restoration.
Dr. Avinesh Bhar notes that many women who present with hormonal insomnia have never been screened for sleep-disordered breathing, which becomes significantly more common after menopause due to the loss of hormonal protection on upper airway muscle tone.
The Hidden Role of Sleep Apnea in Hormonal Insomnia
This is the gap most healthcare providers miss entirely. Estrogen and progesterone exert a protective effect on upper airway muscle tone during sleep. As these hormones decline, women become substantially more vulnerable to obstructive sleep apnea.
Research published in the journal Menopause found that postmenopausal women have a prevalence of sleep apnea that is two to three times higher than premenopausal women of similar anatomy and body composition. Yet this connection is rarely discussed in the clinical management of hormonal insomnia.
When sleep apnea goes undetected, women receive hormonal treatments, cognitive behavioral therapy, or sleep medications that address symptoms without touching the underlying breathing disruption. Fatigue and fragmented sleep persist. The interventions appear to fail. The patient is told to try harder.
A home sleep apnea test can identify whether breathing disruptions are compounding the hormonal sleep disruption. This step is especially critical for women who have tried multiple approaches to hormonal insomnia without sustained improvement.
This home sleep test is often covered by Medicare, Tricare and major insurances and only requires 2-3 nights of sleep testing.


Expert Q&A
Q: I am in perimenopause and cannot sleep through the night. My gynecologist managed my hormones but I still wake up exhausted every morning. What could I be missing?
This is one of the most important questions I hear from patients at Sliiip.com. Hormonal changes are real contributors to sleep disruption, but they are frequently not the only factor. During perimenopause and especially after menopause, women lose the protective hormonal effect on upper airway muscle tone. Sleep apnea becomes significantly more common at exactly the same time other hormonal symptoms are most prominent. If you are waking exhausted despite hormonal management, a sleep evaluation that includes a breathing assessment is an essential next step that most providers have not yet taken.
Dr. Avinesh Bhar Board Certified Sleep Physician Sliiip.com
Cortisol and the 3 a.m. Wake-Up
The cortisol curve is one of the most powerful regulators of your sleep-wake cycle. Under healthy conditions, cortisol rises sharply in the morning to support alertness and declines steadily through the day and evening toward sleep.
Chronic stress, irregular sleep schedules, and metabolic disruption flatten or distort this curve. Elevated evening cortisol prevents the biological wind-down the body needs to initiate sleep. Early morning cortisol surges, sometimes driven by reactive blood sugar drops or a chronically activated stress response, trigger the 3 to 5 a.m. waking that defines hormonal insomnia for many women.
Women experiencing hormonal insomnia are particularly susceptible to cortisol dysregulation. The hormonal shifts of perimenopause and menopause activate the hypothalamic-pituitary-adrenal (HPA) axis, the system that governs cortisol release. Poor sleep elevates cortisol. Elevated cortisol worsens sleep quality. The cycle compounds itself without clinical intervention.
Could it be sleep apnea? Dr. Avinesh Bhar explains this in less than 2 minutes.
Lifestyle Changes That Support Hormonal Sleep Balance
Prioritize consistent sleep and wake times. Going to bed and waking at the same time daily stabilizes the circadian rhythm and reduces cortisol variability. This single behavioral change is the most impactful starting point for hormonal insomnia management. The CDC identifies consistent sleep timing as a foundational sleep hygiene practice.
Manage evening blood sugar. Consuming simple carbohydrates close to bedtime can trigger reactive blood sugar drops that activate the stress response and cause early waking. A small protein-containing snack before bed supports more stable blood sugar through the overnight hours.
Eliminate or reduce alcohol. Alcohol suppresses progesterone activity, disrupts REM sleep, and worsens upper airway instability. Even moderate evening consumption significantly worsens hormonal insomnia outcomes.
Cool the sleep environment. As estrogen declines, the thermoregulatory system becomes less precise. A bedroom temperature between 65 and 68 degrees Fahrenheit supports the core body cooling necessary for deep sleep initiation and maintenance.
Exercise consistently but complete it before evening. Regular physical activity supports cortisol regulation and improves sleep architecture. Exercise within two hours of bedtime elevates core body temperature and cortisol in ways that delay sleep onset.
Is Hormonal Insomnia Controlling Your Nights?
Could an undetected breathing disorder be compounding your hormonal sleep disruption?
Sliiip.com has completed over 10,000 consultations with patients in all 50 states. No referral is needed. Home sleep testing ships directly to your door and is covered by most major insurance plans including Medicare and Tricare.
Frequently Asked Questions
What is hormonal insomnia?
Hormonal insomnia is sleep disruption directly linked to fluctuations in hormones such as estrogen, progesterone, cortisol, and thyroid hormones. It is most common during perimenopause, menopause, the postpartum period, and specific phases of the menstrual cycle. It produces difficulty falling asleep, nighttime waking, and non-restorative sleep.
What are the main symptoms of hormonal insomnia?
Symptoms include difficulty falling asleep, waking multiple times during the night, early morning waking, night sweats, racing thoughts at bedtime, and daytime fatigue that does not resolve with adequate sleep time. Mood changes, cognitive fog, and emotional irritability are also common daytime consequences of hormonal insomnia.
How does estrogen affect sleep quality?
Estrogen supports sleep architecture regulation, including slow-wave and REM sleep. It also supports serotonin production and body temperature regulation. As estrogen declines during perimenopause and menopause, sleep fragmentation increases and deep restorative sleep decreases measurably.
Does progesterone help with sleep?
Yes. Progesterone is converted to a compound that activates GABA receptors in the brain, producing a calming sedating effect. When progesterone drops sharply before menstruation or during perimenopause, this neurological effect diminishes and nighttime wakefulness increases.
Can hormonal changes cause sleep apnea?
The hormonal changes that characterize perimenopause and menopause reduce upper airway muscle tone, significantly increasing the risk of obstructive sleep apnea. Postmenopausal women have two to three times the prevalence of sleep apnea compared to premenopausal women of similar anatomy and weight.
When does hormonal insomnia typically begin?
It often begins during perimenopause, which may start in the early to mid-40s. Some women notice sleep changes tied to their menstrual cycle throughout their reproductive years. It typically intensifies in the years immediately before and after menopause when hormonal fluctuation is most significant.
Can hormonal insomnia affect younger women?
Yes. Women in their 20s and 30s can experience hormonal insomnia tied to the luteal phase of the menstrual cycle when progesterone drops before menstruation. Postpartum hormonal shifts are also a significant trigger for sleep disruption in younger women.
Is melatonin effective for hormonal insomnia?
Melatonin may support sleep timing but does not address the underlying hormonal mechanisms driving disrupted sleep architecture or the sleep-disordered breathing that commonly compounds hormonal insomnia. It is most useful for circadian phase issues rather than the nighttime waking characteristic of hormonal insomnia.
How do I know if my insomnia is hormonal?
Hormonal insomnia typically has a pattern that correlates with menstrual cycle phase, began around perimenopause, or worsened during pregnancy or postpartum. A clinical evaluation that combines a sleep assessment with hormonal screening is the most reliable way to identify the contributing factors.
Can a home sleep test help with hormonal insomnia?
Yes. A home sleep test can identify whether sleep-disordered breathing is compounding hormonal insomnia. This is a critical step for women who have not responded to hormonal or behavioral interventions, as undetected sleep apnea is a common and treatable co-contributor. Learn more at home sleep apnea testing.
What is the most effective approach to hormonal insomnia treatment?
Effective management typically requires addressing both the hormonal component and any underlying sleep disorders simultaneously. This may include hormonal therapy, behavioral sleep interventions, and if a breathing evaluation identifies sleep apnea, targeted treatment for that condition through a board-certified sleep physician.
Does cortisol cause hormonal insomnia?
Elevated or poorly timed cortisol is a significant contributor to hormonal insomnia. It delays sleep onset and triggers early morning waking. Hormonal transitions during perimenopause and menopause activate the hypothalamic-pituitary-adrenal axis, which disrupts the cortisol curve and worsens sleep quality in a compounding cycle.
Latest posts
-
Hormonal Insomnia: Why Your Hormones Are Destroying Your Sleep
Hormonal insomnia refers to sleep disruption driven by fluctuations in estrogen, progesterone, cortisol, and other hormones. It affects millions of women during perimenopause, menopause, pregnancy, and the postpartum period. Hormonal…
-
Silent Sleep Apnea: What It Is and Why It Goes Undiagnosed
Silent sleep apnea is a form of obstructive sleep apnea that produces no audible snoring. It causes repeated breathing pauses during sleep that fragment rest, reduces oxygen levels, and drive…
-
Is Sleep Apnea Genetic? What the Research Says
Yes, sleep apnea has a significant genetic component. Studies estimate that genetics account for approximately 40 percent of the variance in obstructive sleep apnea risk. Inherited traits including craniofacial structure,…
Get updates
Spam-free subscription, we guarantee. This is just a friendly ping when new content is out.

