👉 Register for Free. How to Diagnose Sleep Apnea Faster in Primary Care – FREE Webinar by Dr. Audrey Wells. – Friday, April 24 at 12 PM ET


UARS: The Sleep Disorder Your Doctor Probably Hasn’t Mentioned
UARS sleep disorder is one of the most commonly missed diagnoses in sleep medicine, according to Dr. Avinesh Bhar, Board-Certified Sleep Physician at SLIIIP.com, and many patients spend years being told nothing is wrong with them.
Upper airway resistance syndrome sits in a difficult place when it comes to diagnosis. Patients feel genuinely unwell. Yet their standard sleep studies often come back normal. This leads to years of referrals to cardiologists, psychiatrists, and internists. The actual cause stays unaddressed.
At SLIIIP.com, physicians regularly evaluate patients whose UARS sleep disorder has been missed for years. Sometimes it has been missed for decades. This happens because standard sleep apnea criteria were applied when a more careful analysis was needed.
At SLIIIP.com, the team specializes in exactly these complex and overlooked presentations, with nationwide access and no in person visit required.
SLIIIP’s board certified sleep physicians can do sleep evaluations for sleep apnea. Virtual consultations in all 50 states. Home sleep tests shipped to your door.
SLIIIP’s board-certified sleep physicians can do sleep evaluations for sleep apnea. Virtual consultations in all 50 states. Home sleep tests shipped to your door.
What Is Upper Airway Resistance Syndrome (UARS)?
Upper airway resistance syndrome UARS is a sleep-related breathing disorder that occupies the spectrum between primary snoring and obstructive sleep apnea. In UARS, the upper airway narrows during sleep and creates increased resistance to airflow. This resistance forces the respiratory system to work harder, which triggers brief arousals from sleep arousals that are often too short to be consciously remembered but disruptive enough to destroy the restorative quality of sleep.
The defining characteristic of UARS sleep disorder is this: the breathing events do not fully meet the technical criteria for apnea (complete cessation of airflow) or hypopnea (partial reduction in airflow with associated oxygen desaturation). This is precisely why standard sleep study metrics miss it. A patient with UARS can have an Apnea-Hypopnea Index (AHI) of 3–4 well within the “normal” range and still be experiencing dozens of respiratory effort-related arousals (RERAs) per hour that fragment their sleep architecture just as effectively as untreated sleep apnea.
To accurately identify UARS, a sleep study must use esophageal pressure monitoring or a high-quality nasal pressure transducer capable of capturing RERAs not just the basic oximetry and airflow channels used in standard home sleep tests or entry-level in-lab polysomnography. This technical limitation explains much of the diagnostic gap.
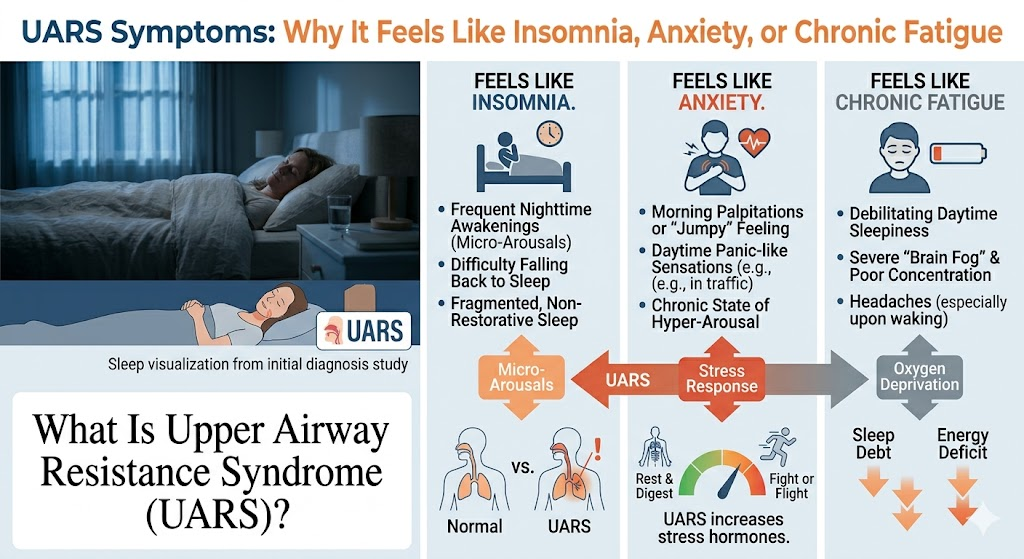
UARS Symptoms: Why It Feels Like Insomnia, Anxiety, or Chronic Fatigue
The symptom profile of UARS sleep disorder is frequently mistaken for a psychiatric or functional disorder, which leads to years of misdirected treatment. Patients with UARS typically present with:
Profound, persistent fatigue. Not just “feeling tired” a bone-deep exhaustion that does not improve with more sleep and is not explained by activity level or stress alone.
Non-restorative sleep. The experience of waking up feeling as though you barely slept, regardless of how many hours you were in bed. Sleep feels light, fragmented, and unrefreshing.
Cognitive difficulties. Brain fog, difficulty concentrating, poor short-term memory, and a general sense of mental sluggishness. These symptoms are often attributed to stress or anxiety but are directly related to fragmented sleep architecture.
Mood disturbances. Increased irritability, emotional sensitivity, and in many cases, symptoms that meet criteria for anxiety or depression which are often treated pharmacologically without ever addressing the sleep disorder driving them.
Morning headaches. Frequent upon waking, related to sleep fragmentation and associated changes in blood pressure and oxygen dynamics overnight.
Postural hypotension and autonomic dysregulation. UARS is associated with dysregulation of the autonomic nervous system, which can manifest as dizziness when standing, temperature regulation difficulties, and a general sense of feeling physically “off” that does not fit a clear medical category.
Snoring (often mild or absent). Unlike classic obstructive sleep apnea, UARS patients may not snore loudly or at all which removes one of the most common clinical flags that prompts a referral for sleep evaluation.
This constellation of symptoms fatigue, brain fog, mood changes, headaches, normal sleep study is the classic UARS presentation. It is also the classic presentation for patients who are repeatedly told that nothing is wrong with them.
UARS vs. Sleep Apnea: Key Differences
Understanding where UARS sits on the spectrum helps clarify why standard approaches to sleep apnea evaluation are insufficient.
In obstructive sleep apnea (OSA), breathing repeatedly stops or significantly reduces during sleep, causing measurable drops in blood oxygen saturation. These events are captured by standard AHI metrics and are unmistakable on a standard sleep study.
In UARS, airflow is restricted but not fully obstructed. The body responds to the increased effort of breathing before the event becomes a full apnea. The result is a RERA, a brief arousal that restores normal breathing before oxygen desaturation occurs. Because oxygen levels stay relatively normal, standard screening metrics miss these events entirely.
The clinical consequence, however, is remarkably similar: sleep fragmentation, impaired sleep architecture, and daytime dysfunction. In some research frameworks, UARS is considered an early point on the same continuum as obstructive sleep apnea rather than a wholly separate entity. From the patient’s perspective, the distinction between UARS and mild untreated sleep apnea is often academic, both cause significant impairment and both warrant clinical evaluation and management.
See Signs of Sleep Apnea and Sleep Apnea Symptoms in Women for related symptom context.

Why Standard Sleep Tests Often Miss UARS
This is the crux of the diagnostic gap, and it is worth understanding in detail.
Standard home sleep tests (HSTs) are designed to identify obstructive sleep apnea using a simplified channel set typically oximetry, airflow, respiratory effort, and body position. They are calibrated to detect apneas and hypopneas using scoring criteria that require either a 3–4% oxygen desaturation or an arousal. RERAs, by definition, often cause arousals without significant desaturation and without esophageal pressure monitoring or sensitive nasal cannula technology, they go uncounted.
Standard in-lab polysomnography (PSG) can detect UARS if the correct analysis is applied specifically, if the technician and interpreting physician are looking for RERAs using esophageal pressure data or validated surrogate measures. However, many sleep lab reports default to AHI as the primary metric, and if AHI is within normal limits, the report may be read as negative without further analysis of RERA burden.
Clinical training gaps. UARS is not universally recognized across all medical specialties, and some physicians do not actively screen for it. This is gradually changing, but the clinical awareness gap remains a practical barrier.
For SLIIIP patients who have had previous “normal” sleep studies but continue to experience symptoms consistent with UARS sleep disorder, a consultation with a physician experienced in the full spectrum of sleep-disordered breathing, not just OSA is the appropriate next step.
Who Gets UARS? Demographics and Risk Factors
UARS has a distinct demographic profile that differs from classic obstructive sleep apnea.
Age: UARS tends to present earlier in life than obstructive sleep apnea. It is not uncommon in young adults in their twenties and thirties.
Sex: Unlike OSA, which disproportionately affects middle-aged men, UARS has a much more equal sex distribution and may be more prevalent in women. This is one reason women with UARS are particularly likely to be misdiagnosed with anxiety, depression, or fibromyalgia.
Body type: UARS patients are often lean or of normal weight. The absence of obesity, a major risk factor for typical OSA removes another clinical flag that might prompt a sleep referral.
Craniofacial anatomy: Structural features such as a narrow palate, small jaw, or high-arched palate can predispose individuals to airway narrowing without the airway collapse pattern typical of obesity-related OSA.
Autonomic nervous system dysregulation: There is growing evidence of an association between UARS and conditions involving autonomic dysfunction, including certain presentations of postural orthostatic tachycardia syndrome (POTS) and chronic fatigue syndrome.
Watch: Sleep apnea sounds

The good news is that the treatments used for obstructive sleep apnea are generally applicable to UARS sleep disorder, often at lower pressure settings or with less intensive intervention.
CPAP and APAP therapy: Continuous or auto-adjusting positive airway pressure is effective for UARS. In many cases, the pressures required are lower than those needed for moderate-to-severe OSA. Some patients with UARS find that CPAP resolves their symptoms dramatically and relatively quickly.
Oral appliances: Mandibular advancement devices that reposition the jaw to open the airway are appropriate for UARS, particularly in patients who are not good CPAP candidates or have mild-to-moderate UARS. See Oral Appliance Sleep Apnea for more detail.
Positional therapy: Some UARS patients have position-dependent symptoms worse on their back, better on their side. Positional devices or behavioral strategies to maintain a lateral sleep position can provide meaningful benefit in these cases.
Nasal and upper airway interventions: Nasal obstruction can worsen upper airway resistance significantly. Addressing nasal valve collapse, septal deviation, or chronic nasal congestion may reduce UARS severity in some patients.
Behavioral and sleep hygiene measures: Alcohol, sedatives, and sleep deprivation all worsen upper airway tone during sleep and can amplify UARS symptoms. These are modifiable factors worth addressing as part of any treatment plan.
When to Ask Your Doctor About UARS
If you recognize yourself in the symptom profile described above particularly if you have had a sleep study that came back “normal” but continue to feel unrested, cognitively impaired, and fatigued the most important step is finding a physician who evaluates the full spectrum of sleep-disordered breathing.
Dr. Avinesh Bhar and the team at SLIIIP.com specialize in diagnostically complex sleep presentations. The SLIIIP model virtual consultations available nationwide, with home sleep testing where appropriate makes it accessible to reach a specialist without navigating a lengthy in-person referral process.
For more on insomnia-like presentations and sleep treatment pathways, see Insomnia Treatment Methods.
At Sliiip, we accept the following insurances:

SLIIIP’s board-certified sleep physicians can do sleep evaluations for sleep apnea. Virtual consultations in all 50 states. Home sleep tests shipped to your door.
Frequently Asked Questions About UARS Sleep Disorder
What does UARS stand for?
Upper airway resistance syndrome a sleep-related breathing disorder in which narrowing of the upper airway during sleep causes repeated brief arousals without meeting the criteria for sleep apnea.
How is UARS different from sleep apnea?
In sleep apnea, breathing stops or significantly reduces with measurable oxygen drops. In UARS, the body responds to increased breathing effort before a full apnea occurs causing arousals that standard tests miss.
Can you have UARS with a normal sleep study?
Yes. Standard sleep studies that rely on AHI often do not capture RERAs, which are the hallmark of UARS. A normal AHI does not rule out UARS.
What are the most common UARS symptoms?
Unrefreshing sleep, persistent fatigue, brain fog, irritability, morning headaches, and difficulty concentrating often without loud snoring.
Who is most likely to have UARS?
Younger adults, women, people with normal body weight, and individuals with narrow craniofacial anatomy are more commonly affected than the typical sleep apnea patient.
Is UARS a real diagnosis?
Yes, though it is not universally recognized in all clinical frameworks. It is well-documented in sleep medicine research and is increasingly recognized as a clinically significant condition.
Can UARS cause anxiety?
Sleep fragmentation from UARS disrupts the nervous system in ways that produce anxiety-like symptoms. Many UARS patients are misdiagnosed with anxiety disorders.
Does UARS cause weight gain?
Fragmented sleep disrupts hormones involved in appetite regulation, which can contribute to weight gain over time, though the effect is generally less pronounced than with moderate-to-severe OSA.
Can children have UARS?
Yes. UARS in children may manifest as behavioral problems, attention difficulties, and poor academic performance often misattributed to ADHD.
What kind of sleep test diagnoses UARS?
An in-lab polysomnography with esophageal pressure monitoring or a high-quality nasal pressure transducer that captures RERAs is the most accurate diagnostic approach.
Does CPAP work for UARS?
Yes. CPAP and APAP therapy are effective for UARS and often require lower pressure settings than for typical OSA.
Can an oral appliance treat UARS?
Oral appliances are a reasonable treatment option for UARS, particularly for patients with mild-to-moderate severity or CPAP intolerance.
Is UARS associated with chronic fatigue syndrome?
There is a recognized association between UARS and chronic fatigue-like presentations, possibly mediated through autonomic nervous system dysregulation.
Does weight loss help UARS?
For patients with anatomy-related UARS, weight loss may have less impact than for obesity-related OSA. Anatomical factors are often the primary driver.
Can UARS be cured?
Treatment can resolve or substantially reduce symptoms. Some surgical interventions (such as procedures to address nasal obstruction or jaw structure) may provide lasting benefit for anatomically-driven cases.
How do I ask my doctor about UARS?
Ask specifically whether your sleep study analyzed respiratory effort-related arousals (RERAs) in addition to AHI. If not, request a referral to a sleep physician experienced in upper airway resistance syndrome.
Is UARS the same as hypopnea?
No. Hypopneas involve a measurable reduction in airflow with associated oxygen desaturation. RERAs in UARS cause arousals before significant desaturation occurs.
Can stress make UARS worse?
Psychological stress increases arousal thresholds and can worsen the symptom burden from UARS. However, UARS is a physical breathing disorder, not a stress-caused condition.
Does UARS affect cardiovascular health?
Research is ongoing, but sleep fragmentation and autonomic dysregulation from UARS may have long-term cardiovascular implications, though typically less severe than moderate-to-severe untreated OSA.
What is the first step if I think I have UARS?
Consult a board-certified sleep physician who evaluates the full spectrum of sleep-disordered breathing, not just OSA. A telemedicine consultation at SLIIIP.com is available in all 50 states.
Thank you for reading this article.
Latest posts
-
Acid Reflux and Sleep Apnea: Why You Wake Up Choking
Acid reflux and sleep apnea show up together far more often than most people expect, and Dr. Avinesh Bhar, Board-Certified Sleep Physician at SLIIIP.com, hears the same story again and…
-
Glymphatic System and Sleep: Your Brain’s Night Wash
The glymphatic system and sleep came into focus about a decade ago when researchers described a fluid pathway that appears to flush waste products through brain tissue, and Dr. Avinesh…
-
Bed Rotting: Real Self-Care or Hidden Exhaustion?
Bed rotting is the name people give to spending a whole day under the covers with snacks, a phone, and no plans, and Dr. Avinesh Bhar, Board-Certified Sleep Physician at…
Get updates
Spam-free subscription, we guarantee. This is just a friendly ping when new content is out.

