👉 Register for Free. How to Diagnose Sleep Apnea Faster in Primary Care – FREE Webinar by Dr. Audrey Wells. – Friday, April 24 at 12 PM ET

Can Sleep Apnea Cause High Blood Pressure? A Doctor Explains
Yes, sleep apnea can cause high blood pressure. Repeated nighttime oxygen drops trigger the sympathetic nervous system to release stress hormones that raise blood pressure during sleep and keep it elevated throughout the day. This connection between sleep apnea and high blood pressure is one of the most clinically documented relationships in sleep medicine.
This article draws on the expertise of Dr. Avinesh Bhar, Board Certified Sleep Physician and Founder of Sliiip.com. Dr. Bhar works with patients across all 50 states via telemedicine and regularly evaluates patients who have spent years treating high blood pressure without ever investigating whether untreated sleep apnea is driving it.
SLIIIP’s board-certified sleep physicians can evaluate whether your high blood pressure is caused by sleep apnea. Virtual consultations in all 50 states. Home sleep tests shipped to your door.
Medical Disclaimer: This article is for educational purposes only. It does not constitute medical advice or a diagnosis. High blood pressure is a serious medical condition. Consult a licensed physician for evaluation and treatment guidance specific to your health history.
The Physiology: How Sleep Apnea Raises Blood Pressure
To understand why sleep apnea causes high blood pressure, it helps to understand what happens in the body during an apnea event.
Obstructive sleep apnea occurs when the upper airway partially or completely collapses during sleep. Breathing stops. Oxygen levels in the blood fall. Carbon dioxide builds up. Within seconds, the brain registers the drop in oxygen and triggers an emergency arousal response.
That arousal response activates the sympathetic nervous system, the same system responsible for the fight-or-flight reaction. Stress hormones including adrenaline and noradrenaline flood the bloodstream. The heart rate accelerates. Blood vessels constrict. Blood pressure spikes.
In a person without sleep apnea, blood pressure naturally decreases by 10 to 20 percent during sleep. This overnight dip is clinically referred to as nocturnal dipping, and it gives the cardiovascular system critical recovery time. In a person with untreated sleep apnea, this dip does not occur. Repeated apnea events keep the sympathetic system activated throughout the night, elevating blood pressure during what should be the most restful period of the cardiovascular cycle.
Learning the signs that your breathing may be affected during sleep is a practical first step. Loud snoring, waking up gasping, morning headaches, and persistent headaches after sleep are all signals worth paying attention to.
The Clinical Evidence
The relationship between sleep apnea and high blood pressure is supported by decades of robust clinical research and is recognized by the American Heart Association and the Joint National Committee on Hypertension (JNC8).
The Wisconsin Sleep Cohort Study, one of the largest population-based investigations of sleep disorders, found that individuals with obstructive sleep apnea had significantly higher rates of hypertension compared to matched individuals without sleep apnea, with a dose-response relationship: more severe apnea produced higher blood pressure elevations.
Critically, this relationship held after controlling for known blood pressure risk factors including obesity, age, alcohol use, and physical activity. Sleep apnea contributed independently to hypertension risk.
Sleep apnea explained by Dr. Avinesh Bhar.
The John Hopkins study, which followed over 6,000 participants, confirmed that even mild sleep apnea was associated with measurable increases in the likelihood of hypertension. The strength of the association increased with apnea severity.
For patients with treatment-resistant hypertension, defined as blood pressure that remains elevated despite three or more antihypertensive medications at adequate doses, studies show that obstructive sleep apnea is present in approximately 70 to 80 percent of cases. Understanding how sleep apnea affects the heart is an important part of managing cardiovascular health comprehensively.
Myth vs. Reality: Sleep Apnea and High Blood Pressure
Myth: If you are treating your high blood pressure with medication, sleep apnea is no longer relevant.
Reality: Antihypertensive medications lower blood pressure by targeting the vascular system. They do not address the overnight sympathetic activation caused by sleep apnea. Treating blood pressure without addressing underlying sleep apnea is like mopping the floor while the tap is still running. The underlying driver remains active.
Myth: Only people with severe sleep apnea develop hypertension.
Reality: The Sleep Heart Health Study found elevated hypertension risk even in patients with mild sleep apnea. Severity correlates with risk, but the relationship exists across the full spectrum of apnea severity.
Myth: Losing weight will fix both the sleep apnea and the high blood pressure.
Reality: Weight management is an important intervention for both conditions, and meaningful weight loss can reduce both AHI scores and blood pressure. However, weight loss does not reliably eliminate either condition in patients with established disease. Clinical evaluation of each condition remains necessary. The relationship between weight and sleep apnea is real but not simple.
Myth: Women do not develop hypertension from sleep apnea as often as men.
Reality: Sleep apnea in women is frequently underdiagnosed because symptoms present differently. Women with undiagnosed sleep apnea carry the same cardiovascular burden from repeated overnight oxygen drops and sympathetic activation. The hypertension risk is present regardless of sex.
Expert Q&A
Q: “I have been on three blood pressure medications for two years and my pressure is still not controlled. My cardiologist has not mentioned sleep apnea. Could this be why?”
“This scenario is incredibly common and it is one of the clearest indications I know of to evaluate sleep apnea. Treatment-resistant hypertension, meaning blood pressure that stays elevated on multiple medications, has a well-documented association with undiagnosed obstructive sleep apnea. In my experience, a meaningful proportion of these patients have never had a sleep study. When we diagnose and treat the sleep apnea, some see blood pressure improvements that years of medication adjustments could not achieve. I am not saying sleep apnea is always the cause, but ruling it out should absolutely be part of the workup. A home sleep test is a fast and non-invasive way to get that answer.”
Dr. Avinesh Bhar Board Certified Sleep Physician Sliiip.com
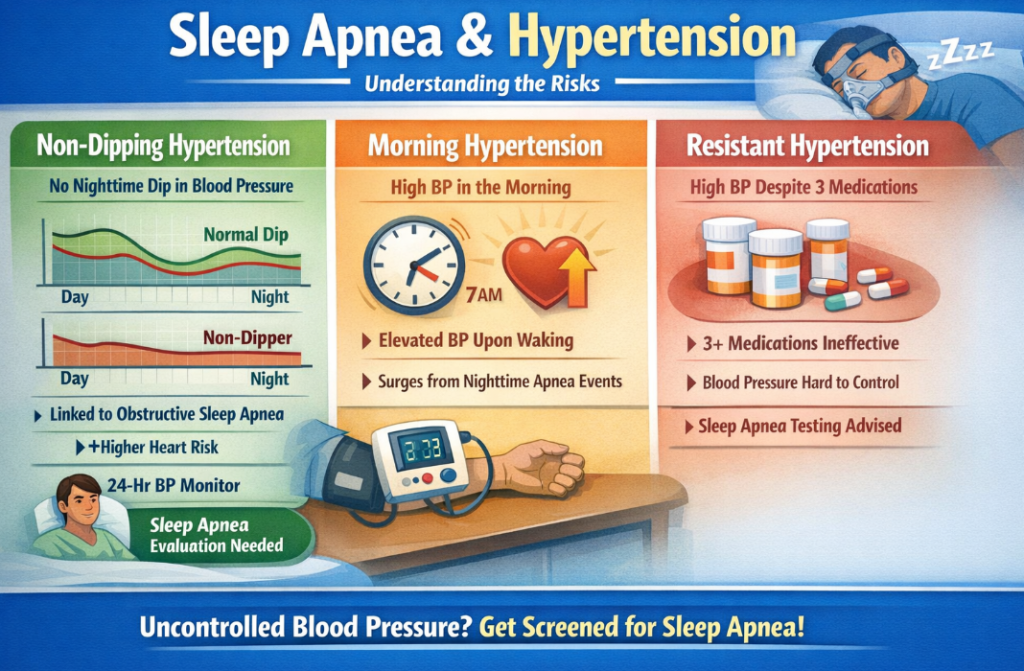
The Specific Types of High Blood Pressure Linked to Sleep Apnea
Not all hypertension presentations have the same relationship to sleep apnea. Certain patterns are particularly strong indicators that sleep-disordered breathing may be a contributing factor.
Non-dipping hypertension. A healthy cardiovascular system shows a measurable overnight dip in blood pressure. Patients whose blood pressure does not dip overnight are called non-dippers. Non-dipping is strongly associated with obstructive sleep apnea and with higher cardiovascular event risk. If a 24-hour ambulatory blood pressure monitor shows a non-dipping pattern, sleep apnea evaluation is warranted.
Morning hypertension. Blood pressure that is highest in the morning, rather than evening, is another pattern associated with overnight sympathetic activation from sleep apnea events. The repeated surges during sleep accumulate and produce elevated readings immediately upon waking.
Resistant hypertension. As noted, the presence of hypertension that does not respond adequately to three antihypertensive medications is one of the strongest clinical triggers for sleep apnea evaluation in cardiovascular medicine.
What Treating Sleep Apnea Does to Blood Pressure?
The evidence on blood pressure outcomes after sleep apnea treatment is encouraging, with important nuances.
CPAP therapy, when used consistently for seven or more hours per night, produces modest but clinically meaningful reductions in both nighttime and daytime blood pressure in patients with obstructive sleep apnea. A meta-analysis published in the Journal of Hypertension found average reductions of approximately 2 to 3 mmHg systolic and diastolic with consistent CPAP use. While modest in absolute terms, these reductions are clinically significant at a population level and are additive to medication effects.

The magnitude of blood pressure reduction is greater in patients with more severe sleep apnea, in patients with treatment-resistant hypertension, and in patients who are non-dippers. These subgroups show the strongest blood pressure response to sleep apnea treatment.
Oral appliance therapy produces similar blood pressure effects to CPAP in patients with mild to moderate apnea, based on comparative studies. For patients who cannot tolerate CPAP, oral appliance therapy is a clinically valid alternative that maintains the cardiovascular benefits of airway management.

The key qualifier in all of this research is treatment adherence. Minimal or inconsistent CPAP use does not produce the same blood pressure benefits as consistent nightly use. This is one reason why working with a sleep physician to optimize treatment and address adherence barriers matters beyond the diagnosis itself.
Recognizing Sleep Apnea in the Context of Hypertension
Many patients with both conditions do not connect them because the signs of sleep apnea are easy to attribute to stress, aging, or busy schedules.
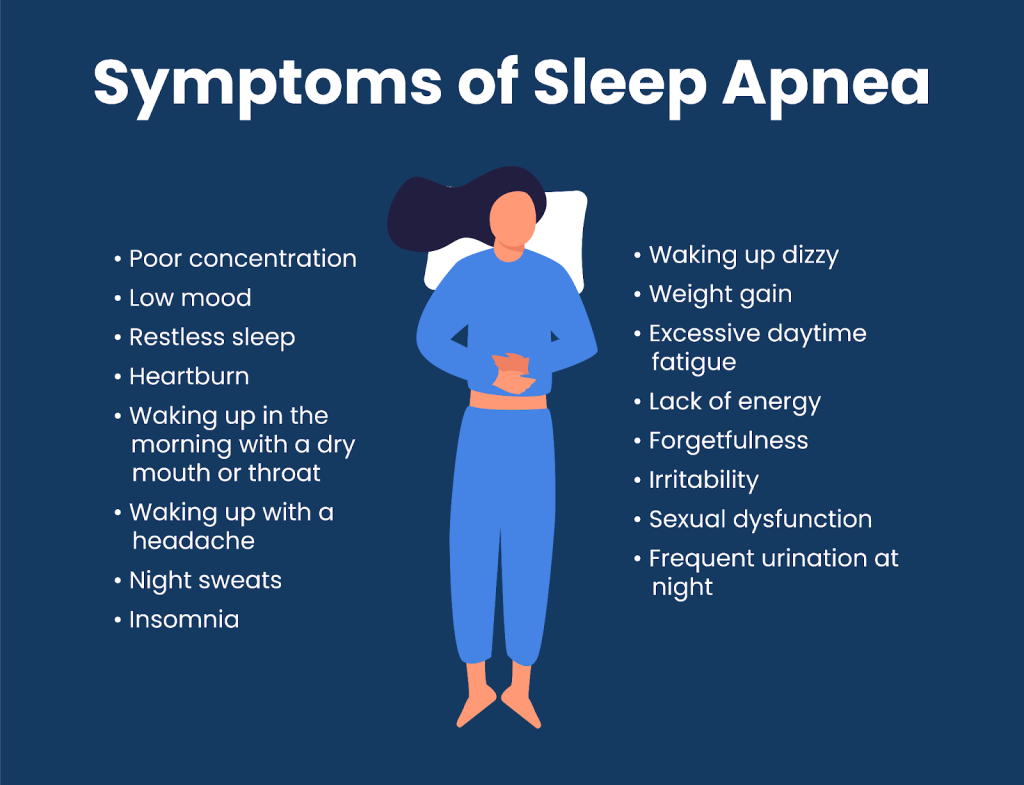
The classic presentation includes loud snoring that has worsened over time, witnessed breathing pauses during sleep, waking up gasping or choking, morning headaches that resolve within an hour of waking, significant daytime sleepiness despite adequate time in bed, and difficulty concentrating.
Women and older adults often present differently, with less obvious snoring and more predominant fatigue, mood changes, and insomnia-like symptoms. Understanding the full range of sleep apnea symptoms is important for recognizing when cardiovascular symptoms may have a sleep-related component.
If you have high blood pressure and recognize any of these patterns in yourself, discussing sleep apnea evaluation with your physician is a reasonable and evidence-supported next step.
Find Out If Sleep Apnea Is Driving Your Blood Pressure
Sliiip.com has completed over 10,000 consultations with patients across all 50 states. No referral is required. A board-certified sleep physician reviews your home sleep test results and helps you understand what your diagnosis means for your cardiovascular health and overall treatment picture.
Most major insurance plans are accepted. Testing is done entirely from home.
Frequently Asked Questions: Sleep Apnea and High Blood Pressure
Can sleep apnea cause high blood pressure? Yes. Sleep apnea causes repeated oxygen drops during sleep that activate the sympathetic nervous system and trigger stress hormone release. This elevates blood pressure during sleep and sustains elevated readings throughout the day. The American Heart Association recognizes obstructive sleep apnea as a recognized contributing cause of hypertension.
How much does sleep apnea raise blood pressure? Untreated obstructive sleep apnea is associated with elevated hypertension risk across the severity spectrum. Systolic blood pressure elevations of 10 mmHg or more have been documented in patients with moderate to severe apnea. Individuals with sleep apnea are two to three times more likely to have hypertension than those without the condition.
Does treating sleep apnea lower blood pressure? Yes, in many patients. Consistent CPAP use is associated with average systolic and diastolic blood pressure reductions of approximately 2 to 3 mmHg based on meta-analyses. Patients with resistant hypertension and non-dipping patterns show the greatest response. Effects are additive to antihypertensive medications.
What is resistant hypertension and how does sleep apnea relate to it? Resistant hypertension is blood pressure that remains elevated despite taking three or more antihypertensive medications at adequate doses. Studies show that obstructive sleep apnea is present in approximately 70 to 80 percent of patients with resistant hypertension, making sleep apnea evaluation a clinical standard in this population.
What is non-dipping blood pressure and is it related to sleep apnea? Non-dipping refers to the absence of the normal 10 to 20 percent overnight blood pressure reduction. It is strongly associated with obstructive sleep apnea and with increased cardiovascular event risk. 24-hour ambulatory blood pressure monitoring can identify this pattern, which is a clinically supported indication for sleep apnea evaluation.
Can CPAP help lower blood pressure? Yes. Research supports that consistent CPAP use reduces both nighttime and daytime blood pressure in patients with obstructive sleep apnea, with the greatest effects seen in patients with more severe apnea and treatment-resistant hypertension. The effect requires adequate nightly CPAP use of seven or more hours.
Is there a link between sleep apnea and heart disease beyond high blood pressure? Yes. Untreated obstructive sleep apnea is independently associated with elevated risk of atrial fibrillation, heart failure, coronary artery disease, and stroke. The mechanism involves chronic sympathetic activation, oxidative stress from repeated oxygen desaturation, and systemic inflammation triggered by the nighttime arousal cycle.
What are the symptoms of sleep apnea in someone with high blood pressure? The overlap symptoms most relevant in hypertensive patients include snoring, morning headaches, daytime fatigue despite adequate sleep time, waking unrefreshed, and witnessed breathing pauses. Non-dipping blood pressure on an ambulatory monitor and treatment-resistant hypertension despite multiple medications are cardiovascular indicators that warrant sleep apnea evaluation.
Does weight loss improve both sleep apnea and blood pressure? Yes, in patients where excess weight contributes to both conditions. Clinically significant weight loss of five percent or more of body weight is associated with reductions in both AHI scores and blood pressure readings in appropriate candidates. Weight management is an important complement to clinical treatment for both conditions but does not eliminate the need for formal evaluation.
How is sleep apnea diagnosed when high blood pressure is present? Diagnosis follows the same pathway regardless of cardiovascular history. A home sleep test worn overnight measures breathing patterns, blood oxygen levels, and heart rate. A board-certified sleep physician interprets the results and generates a formal report including AHI score and severity classification. This report informs both sleep apnea treatment planning and cardiovascular management.
Can sleep apnea cause high blood pressure in women? Yes. The cardiovascular consequences of untreated sleep apnea, including hypertension, apply equally to women. Sleep apnea in women is frequently underdiagnosed because symptoms differ from the classic male presentation. Women with unexplained or resistant hypertension should be evaluated for sleep-disordered breathing as part of a comprehensive cardiovascular workup.
Should cardiologists screen for sleep apnea? Multiple cardiovascular guidelines now recommend sleep apnea screening in patients with resistant hypertension, non-dipping blood pressure, atrial fibrillation, and heart failure. The ACC/AHA and JNC guidelines include sleep apnea as a recognized secondary cause of hypertension that warrants evaluation before a diagnosis of true essential hypertension is finalized.
Latest posts
-
Sleep Apnea During Pregnancy: Signs to Watch For
Sleep apnea during pregnancy is a pattern of pausing or shallow breathing in sleep that, as Dr. Avinesh Bhar, Board-Certified Sleep Physician at SLIIIP.com, explains, can show up as new…
-
Sleep Regularity: Why Consistency Beats Total Hours
Sleep regularity, meaning the habit of falling asleep and waking up at close to the same time each day, is a pattern that Dr. Avinesh Bhar, Board-Certified Sleep Physician at…
-
Narcolepsy Symptoms: Early Signs and When to Get Tested
Narcolepsy symptoms can hide behind years of ordinary tiredness, which is why Dr. Avinesh Bhar, Board-Certified Sleep Physician at SLIIIP.com, urges anyone battling relentless daytime sleepiness to learn the warning…
Get updates
Spam-free subscription, we guarantee. This is just a friendly ping when new content is out.

