👉 Register for Free. How to Diagnose Sleep Apnea Faster in Primary Care – FREE Webinar by Dr. Audrey Wells. – Friday, April 24 at 12 PM ET


Is My Depression Actually a Sleep Problem?
You are exhausted all the time. You have lost interest in things you used to enjoy. Concentrating feels impossible. Your mood is flat, or worse. Your doctor diagnosed depression but you may be wondering, “Is my depression actually a sleep problem?”
Here is what most people are never told: the symptoms of depression and the symptoms of a sleep disorder overlap almost completely. Dr. Avinesh Bhar, the Founder of SLIIIP, sees many of these symptoms in his sleep disorder patients. Fatigue, low motivation, poor concentration, irritability, weight changes, and mood disruption are hallmarks of depression with a sleep disorder.
The Overlap That Leads to Misdiagnosis
Consider the symptoms of untreated obstructive sleep apnea: excessive daytime sleepiness, morning headaches, difficulty concentrating, irritability, low motivation, weight gain, decreased libido, and a general feeling of not being yourself. Now consider the diagnostic criteria for major depressive disorder. The overlap is striking.
Studies show that up to 75% of people with depression also have sleep problems, and people with insomnia are up to 10 times more likely to develop depression. Research published in PMC found that sleep disturbances often precede depressive episodes and can persist even after other symptoms improve. Unresolved sleep problems are one of the strongest predictors of depression relapse.
Perhaps most importantly, in a significant subset of patients diagnosed with depression, the primary driver is an undiagnosed and untreated sleep disorder. When the sleep disorder is treated, depressive symptoms improve or resolve entirely.
How Sleep Apnea Mimics Depression
Fragmented sleep reduces deep and REM sleep. Both stages are essential for emotional regulation and cognitive function. When apnea fragments these stages night after night, mood deteriorates, concentration suffers, and motivation disappears. Many patients sleep 8 hours and still feel tired, never suspecting their airway is the problem.
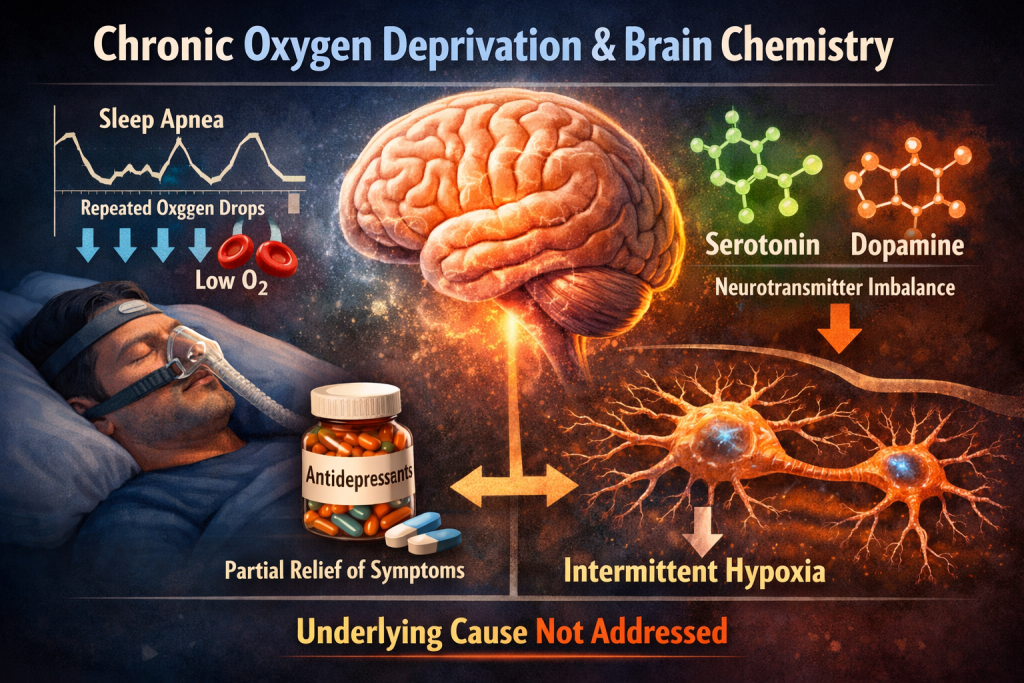
Chronic oxygen deprivation affects brain chemistry. Repeated oxygen drops during sleep can alter neurotransmitter levels, including serotonin and dopamine, the same neurotransmitters targeted by antidepressants. If the root cause is intermittent hypoxia, an antidepressant may partially improve symptoms but cannot address the underlying physiology. This oxygen disruption also contributes to severe brain fog that patients frequently report.
Sleep apnea disproportionately affects demographics already at higher risk for depression.
Women in perimenopause and menopause, older adults, and people with chronic health conditions are at elevated risk for both conditions, making it harder to distinguish one from the other without a proper sleep evaluation.
That’s where a sleep dentist can play an important role. Trained in dental sleep medicine, a sleep dentist can help identify signs of obstructive sleep apnea and discuss treatment options, including custom oral appliance therapy.

These small, comfortable devices are worn at night to gently reposition the jaw and keep the airway open, offering an effective alternative for many patients who cannot tolerate CPAP. Recognizing the signs of sleep apnea and understanding available treatment options is a critical first step toward accurate diagnosis and better sleep health.
Below a sleep dentist answers common questions related to sleep apnea and oral appliance.
Hans Schleicher, DDS, D-IAOS
https://sleephouston.com/
1) They don’t think they have sleep apnea
Many patients that we see have no idea that they have sleep apnea and just assume that their symptoms are just the natural course of getting older. The symptoms can be subtle enough to not rise to the point of alarm in the patient. After educating the patient about the negative consequences of not treating OSA we refer the patient to a sleep testing company for evaluation and then follow up with another explanation consultation to discuss the next steps.
2) They think the oral appliance will be uncomfortable
Reassurance is given to the patient. Dr. Schleicher has been wearing and appliance for over 20 years and can personally attest to its ease of use and comfort. Knowing that virtually all of our patients are able to wear the appliance every night for 8 hours 7 nights a week is also reassuring to the patient.
3) They wonder if they have to wear the oral appliance all their life?
We remind the patient that we are not curing OSA, but we are treating OSA, and just as in CPAP it is something they will do for the rest of their life. Our experience with our patients is that once they have been successfully titrated with the appliance to the maximum medical benefit they are 100% compliant because they feel so much better when they wear the appliance.
4) How many years can an oral appliance last?
The appliance’s durability is very good. The appliances have a 3 years warranty for any breakage. It is not uncommon for the patients to be able to use the same appliance over 6-7 years with proper care.
5) Does insurance cover oral appliances?
Medicare and most private medical insurance companies cover oral appliances CPT code E0486 when documented with a medical grade sleep test interpreted by an MD, with a written prescription and letter of medical necessity. MDs are concerned for their patients and work well with us in the documentation process.
6) Is it more comfortable than CPAP?
Oral appliances are consistently rated by our patients as more comfortable that CPAP by a wide margin. CPAP failure with patients is mostly related to their comfort during sleep.Oral appliances have a 98% compliance rate and is generally recognized as a superior treatment for patients as an FDA approved alternative to CPAP for those who are intolerant or refuse CPAP treatment.
The Bidirectional Relationship: It Goes Both Ways
Sleep problems can cause depression. Chronic insomnia, sleep apnea, and other disorders deprive the brain of restorative sleep, leading to mood, cognitive, and motivational changes that define depression. People with persistent insomnia have significantly elevated risk of a first depressive episode. Understanding the importance of sleep is essential for sleep and mental health.
Depression can worsen sleep. Depression alters sleep architecture: more light sleep, less deep sleep. It causes early morning awakening (4 or 5 AM, unable to return to sleep). Rumination and hopelessness create conditioned arousal.
Treating one often improves the other. This is the most actionable insight. Treating insomnia (with CBT-I) in people with comorbid depression improves depressive symptoms. Treating sleep apnea in depressed patients often leads to meaningful mood improvement. In some cases, treating the sleep disorder is the single most impactful intervention.
What to Do If You Suspect Your Depression Is Sleep-Related
Step 1: Ask about sleep in your mental health appointments. Make sure your provider has asked about snoring, nighttime waking, morning headaches, daytime sleepiness, and whether sleep feels restorative. If not, bring it up.
Step 2: Get a sleep evaluation. A board-certified sleep medicine physician can assess whether a sleep disorder is contributing. This can be done via telemedicine. A home sleep test screens for obstructive sleep apnea without a sleep lab visit.
Step 3: Coordinate care. The best outcomes occur when sleep medicine and mental health providers work together. If sleep apnea is diagnosed, treatment (CPAP or oral appliance) can be initiated alongside depression treatment. Many patients find depressive symptoms improve significantly once sleep quality improves.
The Menopause Connection
Menopause is a convergence point for sleep problems and depression. Declining estrogen and progesterone levels disrupt sleep architecture, increase sleep apnea risk (by reducing airway muscle tone), cause hot flashes and night sweats that fragment sleep, and directly affect mood regulation.
Women in perimenopause and menopause are at elevated risk for both new-onset depression and new-onset sleep apnea. A sleep evaluation is particularly important for women in this age group who develop depressive symptoms, as treating a newly identified sleep disorder can dramatically improve mood and quality of life. Taking a sleep disorder quiz can help determine if further evaluation is warranted.
Could a Sleep Disorder Be Contributing to Your Depression? SLIIIP’s board-certified sleep medicine physicians specialize in identifying sleep disorders that mimic or worsen depression. Virtual consultations in all 50 states. Home sleep tests shipped to your door. Results sent to your referring provider. |
Frequently Asked Questions
Can a sleep disorder cause depression?
Yes. Chronic sleep disorders including insomnia, obstructive sleep apnea, and restless legs syndrome can cause or significantly worsen depression. Sleep deprivation disrupts serotonin and dopamine regulation, impairs emotional processing, and reduces stress management capacity. Research from Johns Hopkins reports that people with insomnia are up to 10 times more likely to develop depression.
Why do antidepressants not help my sleep?
Many antidepressants alter sleep architecture. Some SSRIs suppress REM sleep. Others are stimulating and worsen insomnia. Additionally, if depression is driven by undiagnosed sleep apnea, an antidepressant addresses the symptom (mood) but not the cause (disrupted breathing). Treating the sleep disorder alongside depression often produces better outcomes.
Is my insomnia causing my depression, or is my depression causing my insomnia?
It can work either direction, and often both are contributing. Research shows insomnia often precedes depressive episodes by months or years, suggesting poor sleep can be a causal factor. Depression also disrupts sleep through altered chemistry and rumination. The practical takeaway: treat both simultaneously for the best results. An effective insomnia treatment plan can make a meaningful difference.
Can treating sleep apnea improve depression?
Yes. Multiple studies demonstrate that treating OSA with CPAP or oral appliance therapy leads to meaningful improvement in depressive symptoms. A systematic review published in PLOS Medicine found that CPAP significantly reduced depression scores in patients with comorbid OSA and depression. Patients report improved mood, energy, motivation, and cognitive clarity.
What are the signs that my depression might actually be a sleep problem?
Warning signs include: you feel exhausted no matter how much you sleep; depression worsened gradually rather than after a triggering event; you snore or have been told you stop breathing during sleep; you wake with morning headaches or dry mouth; you have gained weight without clear dietary change; antidepressants have not fully resolved symptoms; you fall asleep easily but wake unrefreshed.
What is the link between sleep apnea and serotonin?
Obstructive sleep apnea causes repeated oxygen drops (intermittent hypoxia). Research suggests chronic intermittent hypoxia can reduce brain serotonin levels. Since serotonin is a key mood-regulating neurotransmitter, this may be one mechanism by which untreated sleep apnea produces depressive symptoms. Restoring normal oxygenation through treatment may help normalize serotonin over time. Untreated sleep apnea also takes a toll on cardiovascular health.
Can a home sleep test detect why I am depressed?
A home sleep test does not diagnose depression. It detects obstructive sleep apnea and breathing-related sleep disorders that may be causing or worsening depressive symptoms. If significant sleep-disordered breathing is found, treating it can lead to mood improvement. Think of it as ruling in or ruling out a treatable physical cause.
Is depression worse with poor sleep?
Yes. Poor sleep consistently worsens depression. The American Psychiatric Association reports that residual insomnia after depression treatment is one of the strongest relapse predictors. Sleep deprivation impairs emotional regulation, amplifies negative thoughts, reduces motivation, and increases suicidal ideation. Addressing sleep is critical to effective depression treatment.
Can oral appliance therapy help with depression?
If depression is driven or worsened by untreated sleep apnea, an oral appliance can help by restoring normal breathing during sleep. This improves sleep quality, reduces oxygen deprivation, and normalizes stress hormone levels. Devices like the myTAP oral appliance are a non-invasive option. It is not a treatment for depression itself, but for the sleep disorder that may be fueling it. Coordinate with your mental health provider.
What is the relationship between sleep, depression, and menopause?
Menopause is a convergence point. Declining estrogen and progesterone disrupt sleep architecture, increase sleep apnea risk (reduced airway muscle tone), cause hot flashes and night sweats that fragment sleep, and directly affect mood regulation. Women in perimenopause and menopause are at elevated risk for both new-onset depression and new-onset sleep apnea. A sleep evaluation is particularly important for this group.
Should I see a sleep doctor or a psychiatrist for depression with sleep problems?
Ideally, both. A sleep physician evaluates whether a sleep disorder is contributing. A psychiatrist or therapist addresses psychological components. The most effective plans are coordinated. Telemedicine sleep services like SLIIIP make it easy to add a sleep evaluation without replacing existing mental health care.
Can fixing my sleep cure my depression?
“Cure” is a strong word, and depression is complex with multiple factors. However, for patients whose depression is primarily driven by a sleep disorder, treating the sleep problem can produce dramatic mood, energy, and functioning improvements. For others, treating sleep will not eliminate depression but will improve treatment response and reduce relapse risk. Either way, addressing sleep is one of the most impactful steps you can take.
Latest posts
-
Bed Rotting: Real Self-Care or Hidden Exhaustion?
Bed rotting is the name people give to spending a whole day under the covers with snacks, a phone, and no plans, and Dr. Avinesh Bhar, Board-Certified Sleep Physician at…
-
Bedtime Stacking: Is Your Night Routine Too Long?
Bedtime stacking happens when a wind-down routine keeps growing until it swallows a full hour of the evening, and Dr. Avinesh Bhar, Board-Certified Sleep Physician at SLIIIP.com, hears about it…
-
Digital Sunset: Build a Low-Tech Bedroom for Sleep
A digital sunset, the simple habit of powering down screens and dimming light well before bed, is a routine Dr. Avinesh Bhar, Board-Certified Sleep Physician at SLIIIP.com, often suggests to…
Get updates
Spam-free subscription, we guarantee. This is just a friendly ping when new content is out.

