👉 Register for Free. Can Your Dentist Spot Sleep Apnea? – Webinar by Dr. Michael DeLuke & Dr. Avinesh Bhar. – Friday April 10 at 11AM EST


Sleep Apnea in Children: Early Signs and When to Get Help
When most people think about sleep apnea, they picture an adult. But sleep apnea in children is far more common than many parents realize, and it often goes unidentified for months or years because the signs can look very different in a child than in a grown adult. A child with sleep-disordered breathing does not always snore loudly or gasp in an obvious way. The signals are sometimes subtler: restless nights, unexplained behavioral changes, difficulty concentrating at school, or simply a child who never seems properly rested no matter how many hours they sleep.
This guide covers the early warning signs parents should know, the risk factors that make some children more likely to develop sleep-disordered breathing, and when it is appropriate to speak with a physician about an evaluation.
SLIIIP’s board-certified sleep physicians can do sleep evaluations for sleep apnea. Virtual consultations in all 50 states. Home sleep tests shipped to your door.
What Is Sleep Apnea in Children?
Pediatric sleep apnea, more precisely called pediatric obstructive sleep apnea (OSA), occurs when the upper airway becomes partially or fully blocked during sleep, interrupting normal breathing. These interruptions can last several seconds, and they typically end with a brief arousal that brings the child back to a lighter sleep stage, often without the child or their parents being aware it has happened.

The result is sleep that is fragmented at a physiological level even when it appears continuous from the outside. A child may sleep for nine or ten hours and still wake feeling unrestored, because the quality of that sleep, not just the quantity, has been repeatedly disrupted by breathing events.
Take the Child Sleep Apnea Quiz
Pediatric OSA differs from adult OSA in several important ways. In adults, obesity and anatomical changes associated with aging are the most common contributors. In children, enlarged tonsils and adenoids are the most frequent anatomical cause, which is why pediatric sleep apnea is more common in younger children and often improves significantly after a tonsillectomy.
For a broader understanding of what sleep apnea involves across all ages, the complete guide to sleep apnea covers the condition in full.
How Common Is Sleep Apnea in Children?
Research estimates suggest that obstructive sleep apnea affects somewhere between 1 and 5 percent of children, with the peak prevalence occurring in the preschool and early school-age years, roughly between ages two and eight, when tonsil and adenoid tissue tends to be largest relative to the size of the airway. However, sleep-disordered breathing on a spectrum, including habitual snoring and upper airway resistance without frank apnea, is thought to be considerably more prevalent.
Many cases go unrecognized for extended periods. Parents often assume nighttime snoring is harmless, daytime behavioral symptoms are attributable to personality or attention-related issues, or that their child simply is not a good sleeper. Awareness of what the actual early indicators look like is the most important factor in shortening the time between onset and evaluation.

Early Signs of Sleep Apnea in Children
The following signs are among the most commonly reported in children later confirmed to have sleep-disordered breathing. No single sign is definitive on its own, but a pattern of several of them occurring together warrants a conversation with your child’s physician.
Loud or Frequent Snoring
Occasional light snoring in children is common and not necessarily a cause for concern. Loud, habitual snoring that occurs on most nights, particularly snoring that is audible from outside the child’s closed bedroom door, is a more meaningful indicator. Snoring reflects partial obstruction of the upper airway during sleep and is one of the most consistent early signals of sleep-disordered breathing in the pediatric population.
Pauses in Breathing During Sleep
If you have ever watched your child sleep and noticed them stop breathing for several seconds before resuming with a gasp, snort, or sudden movement, that is an observable apnea event. This is one of the most direct indicators of obstructive sleep apnea and should prompt a conversation with your pediatrician. Not all events are this visible, but when they are, they are significant.
Restless Sleep and Unusual Sleep Positions
Children with sleep-disordered breathing often move more than other children during sleep, shifting position frequently in an unconscious effort to maintain an open airway. Some children develop a pattern of sleeping with their neck extended or their head hyperextended backward over the edge of a pillow, a posture that widens the upper airway and reflects an instinctive compensation for airway restriction.
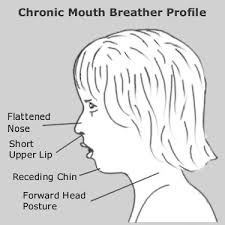
Mouth Breathing During Sleep
Breathing through the mouth during sleep, rather than through the nose, is common in children with enlarged tonsils or adenoids that partially block the nasal airway. You may notice your child sleeping with their mouth consistently open, or waking with a dry mouth. Mouth breathing during sleep is not always associated with sleep apnea, but in combination with other signs it is worth noting.
Night Sweats
Increased effort to breathe against a partially obstructed airway is physically demanding, even during sleep. Children who work harder to breathe throughout the night may sweat significantly more than other children despite normal room temperatures. Frequent night sweats not explained by fever or excessive bedding are a commonly reported but underappreciated early sign.
Bedwetting After Being Dry
Secondary enuresis, the return of bedwetting in a child who had previously been consistently dry, has been associated with sleep-disordered breathing in research literature. The mechanism is thought to involve altered secretion of antidiuretic hormone during disrupted sleep. If a child who was dry for an extended period begins wetting the bed again without another obvious explanation, sleep quality is worth investigating.
Daytime Behavioral Changes
This is one of the most important and most overlooked areas. In adults, sleep apnea typically presents as excessive daytime sleepiness. In children, the daytime manifestation is often the opposite: hyperactivity, impulsivity, irritability, and difficulty regulating attention. Children with untreated sleep-disordered breathing are sometimes misidentified as having attention-deficit hyperactivity disorder (ADHD), because the behavioral presentation overlaps considerably. If your child is showing behavioral changes at home or school that are difficult to explain, sleep quality is a factor worth exploring with your pediatrician.
Difficulty Waking in the Morning
A child who is genuinely difficult to wake in the morning despite having slept for an appropriate duration, and who remains visibly groggy, irritable, or uncoordinated for an extended period after waking, may not be getting restorative sleep. This pattern, particularly when it contrasts with a child who was previously easy to wake, is worth noting.
Poor School Performance or Concentration
Sleep is essential for memory consolidation, sustained attention, and cognitive processing. Children whose sleep is fragmented by breathing disruptions may show declining academic performance, difficulty sustaining attention in class, or problems retaining information they were previously able to hold. Teachers sometimes report these changes before parents identify them at home.
Risk Factors for Sleep Apnea in Children
While any child can develop sleep-disordered breathing, certain factors increase the likelihood. Being aware of these can help parents decide whether to discuss screening with their pediatrician even in the absence of obvious symptoms.
Enlarged tonsils and adenoids. This is the most common anatomical risk factor in the pediatric age group. Tonsil and adenoid tissue naturally reaches its largest size relative to the airway in early childhood, and when it is unusually large, it can significantly narrow the pharyngeal airway during sleep.
SLIIIP’s board-certified sleep physicians can do sleep evaluations for sleep apnea. Virtual consultations in all 50 states. Home sleep tests shipped to your door.

Obesity. Excess adipose tissue around the neck and throat can contribute to airway narrowing during sleep in children just as it does in adults. The rising prevalence of childhood obesity is thought to be contributing to an increase in pediatric OSA diagnoses.
Craniofacial differences. Structural differences in the jaw, palate, or midface, including conditions such as Down syndrome, Pierre Robin sequence, or simply a naturally small or recessed jaw, can reduce the space available in the upper airway during sleep.
Family history. Sleep apnea has a heritable component, and children with a parent or sibling who has been diagnosed with sleep-disordered breathing have a higher likelihood of developing it themselves.
Allergies and chronic nasal congestion. Chronic nasal obstruction from allergic rhinitis forces habitual mouth breathing, which alters the muscle tone patterns of the pharynx during sleep and may increase the risk of airway collapse.
Prematurity. Children born prematurely have a higher incidence of sleep-disordered breathing in early childhood, related to developmental differences in the respiratory control systems that mature through the neonatal period.
The full spectrum of warning signs across the age range is covered in the guide to obstructive sleep apnea warning signs, which includes both pediatric and adult presentations.
How Is Sleep Apnea Diagnosed in Children?
The standard diagnostic tool for pediatric OSA is an overnight polysomnography, typically conducted in a pediatric sleep laboratory. This in-lab study captures a comprehensive range of physiological data including brain wave activity, eye movements, muscle tone, oxygen levels, airflow, and respiratory effort, providing the detailed picture needed to characterize sleep-disordered breathing in a developing child.
Home sleep testing, which is widely used for adult OSA evaluation, is less standardized in the pediatric population. Many pediatric sleep medicine specialists prefer in-lab studies for children due to the greater complexity of interpreting sleep-disordered breathing in a developing respiratory system and the importance of capturing sleep staging data. Your child’s physician will advise on the appropriate evaluation type based on your child’s age, symptom profile, and overall health picture.
If you suspect your child may have sleep-disordered breathing, the most appropriate first step is a conversation with your pediatrician, who can perform an initial assessment including examination of the tonsils and adenoids, and provide a referral to a pediatric sleep medicine specialist or ENT if warranted.
For parents who want to explore whether their child’s symptoms warrant further attention, the does my child have sleep apnea quiz is a useful starting point for framing the conversation with your child’s doctor.
What Happens If Pediatric Sleep Apnea Goes Unaddressed?
Untreated sleep-disordered breathing in children is associated with a range of developmental and health concerns. Growth is one area that has received significant research attention: growth hormone is secreted primarily during deep sleep, and children whose sleep is chronically fragmented may show impaired growth patterns. Cardiovascular effects, including elevated blood pressure, have also been documented in children with untreated OSA. Neurobehavioral outcomes, including sustained attention difficulties, behavioral regulation, and academic performance, are among the most consistently reported consequences in the literature.
The encouraging counterpart to this picture is that many children show meaningful improvement in behavioral symptoms, school performance, and sleep quality following appropriate intervention. Early identification matters.
Concerned about your child’s sleep?
Start with the quiz designed to help parents identify whether their child’s symptoms warrant a clinical conversation.
Take the Child Sleep Apnea Quiz
What About Adult Sleep Apnea in the Family?
It is worth noting that if a parent is being evaluated for their own sleep-disordered breathing, this is a natural opportunity to consider whether their children may also be at risk. Sleep apnea has a heritable component, and households where one or both parents have been diagnosed with OSA should be aware that their children warrant monitoring for relevant signs, particularly if any of the risk factors described above are present.
SLIIIP’s clinical team, led by sleep medicine physician Dr. Avinesh Bhar, evaluates adults through a fully online telemedicine platform. For pediatric evaluation needs, the appropriate route is through your child’s primary care physician and, if indicated, a referral to a pediatric sleep or ENT specialist.
Concerned about your own sleep?
Adults in the household can complete a home sleep test from their own bed. Results reviewed by a board-certified physician within days.
SLIIIP’s board-certified sleep physicians can do sleep evaluations for sleep apnea. Virtual consultations in all 50 states. Home sleep tests shipped to your door.
Frequently Asked Questions About Sleep Apnea in Children
Can children have sleep apnea?
Yes. Sleep apnea is estimated to affect between 1 and 5 percent of children, with the highest prevalence in the preschool and early school-age years. It is more common than many parents and physicians realize.
What causes sleep apnea in children?
The most common cause in young children is enlarged tonsils and adenoids that partially block the upper airway during sleep. Obesity, craniofacial structural differences, chronic nasal congestion, and a family history of sleep apnea are also recognized risk factors.
What does sleep apnea look like in a child?
Sleep apnea in children may present as loud habitual snoring, observed pauses in breathing during sleep, restless sleep, mouth breathing, night sweats, daytime hyperactivity or irritability, difficulty concentrating, or problems waking in the morning despite adequate sleep duration.
How is sleep apnea different in children versus adults?
In adults, sleep apnea most commonly presents as excessive daytime sleepiness. In children, the daytime manifestation is more often hyperactivity, behavioral dysregulation, and attention difficulties. The anatomical causes also differ, with enlarged tonsils and adenoids being the primary driver in children rather than obesity or age-related tissue changes.
Does my child need a sleep study to diagnose sleep apnea?
An overnight polysomnography, typically conducted in a pediatric sleep laboratory, is the standard diagnostic test for pediatric OSA. Your child’s physician will advise on whether a referral for sleep testing is appropriate based on the clinical picture.
Can children outgrow sleep apnea?
Some children, particularly those whose OSA is primarily related to enlarged tonsils and adenoids, may show improvement as they grow and those structures shrink relative to the size of the airway. However, waiting without evaluation or intervention carries the risk of developmental consequences during the period the condition goes unmanaged.
Can sleep apnea in children cause behavioral problems?
Research consistently links untreated pediatric OSA with behavioral dysregulation, impulsivity, hyperactivity, and attention difficulties that can resemble ADHD. Addressing the underlying sleep-disordered breathing in these cases is associated with improvements in behavioral outcomes.
Is snoring always a sign of sleep apnea in children?
Not always. Occasional light snoring can occur in otherwise healthy children, particularly during upper respiratory infections. Habitual loud snoring that occurs on most nights is more likely to warrant evaluation, especially when accompanied by other signs such as restless sleep, observed breathing pauses, or daytime behavioral changes.
Can a child have sleep apnea without snoring?
Yes. Not all children with sleep-disordered breathing snore loudly. Some present primarily with restless sleep, unusual sleep positions, daytime behavioral symptoms, or poor growth without prominent snoring. The absence of obvious snoring does not rule out sleep-disordered breathing.
What age can children develop sleep apnea?
Sleep apnea can develop at any age in childhood, including infancy. The peak prevalence is in the preschool and early school-age years, roughly ages two through eight, when tonsil and adenoid tissue tends to be largest relative to airway size.
How is pediatric sleep apnea managed?
Management depends on the underlying cause and severity. Adenotonsillectomy is a common first-line option when enlarged tonsils and adenoids are the primary contributor. Other approaches may include positional therapy, nasal decongestant treatment for allergy-related congestion, weight management, or in selected cases, CPAP therapy. Your child’s specialist will recommend an approach based on the specific clinical findings.
Does CPAP work for children with sleep apnea?
CPAP therapy can be used in children when anatomical surgery is not possible or has not fully resolved the breathing disruption. Pediatric CPAP involves age-appropriate mask sizes and pressure settings and typically requires a period of acclimatization. Not all children are candidates, and the decision is made in consultation with a pediatric sleep specialist.
Can enlarged tonsils cause sleep apnea?
Yes. Enlarged palatine tonsils and adenoids are the most common anatomical cause of obstructive sleep apnea in young children. When these tissues are large relative to the size of the pharyngeal airway, they can significantly restrict airflow during sleep, particularly when muscle tone relaxes in deeper sleep stages.
What should I do if I suspect my child has sleep apnea?
Start with your child’s primary care physician or pediatrician. Describe the signs you have observed, when they began, and how frequently they occur. Your physician can perform an initial examination and, if warranted, refer your child to a pediatric sleep medicine specialist or ENT for further evaluation.
Is there a quiz I can take to assess my child’s sleep apnea risk?
Yes. The does my child have sleep apnea quiz is designed to help parents identify whether their child’s symptoms warrant a clinical conversation. It is not a diagnostic tool but provides a structured way to assess whether further evaluation is appropriate.
Can allergies cause sleep apnea in children?
Chronic nasal congestion from allergic rhinitis can contribute to sleep-disordered breathing by obstructing nasal airflow and promoting habitual mouth breathing, which alters upper airway muscle tone patterns. Managing allergic rhinitis is sometimes part of a broader approach to improving sleep breathing in affected children.
What is the relationship between sleep apnea and ADHD in children?
The behavioral symptoms of untreated pediatric sleep apnea, including hyperactivity, impulsivity, and inattention, overlap considerably with the diagnostic criteria for ADHD. Research suggests that some children diagnosed with ADHD may have underlying sleep-disordered breathing as a contributing or primary cause of their symptoms. Evaluating sleep in children with behavioral concerns is increasingly recognized as clinically important.
Does sleep apnea affect a child’s growth?
Growth hormone is secreted primarily during deep sleep stages. Chronic sleep fragmentation caused by sleep-disordered breathing can interfere with this secretion pattern. Research has documented associations between untreated pediatric OSA and impaired growth, with some studies showing catch-up growth following adenotonsillectomy.
Can a child’s sleep apnea affect their heart?
Research has documented cardiovascular effects of untreated pediatric OSA, including elevated blood pressure and changes in cardiac function in some studies. These findings reinforce the importance of timely evaluation and management rather than a wait-and-see approach.
Is sleep apnea in children related to bedwetting?
Secondary enuresis, the return of bedwetting in a child who was previously dry, has been associated with sleep-disordered breathing in several studies. The proposed mechanism involves altered secretion of antidiuretic hormone during disrupted sleep. Persistent or unexplained bedwetting is worth including in a conversation with your child’s physician.
Thank you for reading this article.
Latest posts
-
Inspire Sleep Apnea Device: Is the Implant Right for You? A Physician Explains
Inspire sleep apnea devices are often overlooked as a treatment option, according to Dr. Avinesh Bhar. Board-Certified Sleep Physician at SLIIIP.com, even among patients who have struggled with CPAP for…
-
Magnesium for Sleep: Does It Actually Work? A Sleep Doctor Explains
Magnesium for sleep is often overlooked, according to Dr. Avinesh Bhar. Board-Certified Sleep Physician at SLIIIP.com, many individuals experience symptoms without clear awareness. Despite being the most-searched sleep supplement of…
-
Positional Sleep Apnea: What It Is and What May Help
Not everyone with obstructive sleep apnea experiences the same number of breathing disruptions regardless of how they sleep, according to Dr. Avinesh Bhar. For a significant proportion of people with…
Get updates
Spam-free subscription, we guarantee. This is just a friendly ping when new content is out.

