👉 Register for Free. How to Diagnose Sleep Apnea Faster in Primary Care – FREE Webinar by Dr. Audrey Wells. – Friday, April 24 at 12 PM ET


Sleep Apnea Without CPAP: 6 Alternatives That Actually Work
Sleep apnea treatment without CPAP is not only possible, it is clinically supported. For patients who cannot tolerate CPAP or are seeking alternatives, options including oral appliance therapy, positional therapy, weight management, myofunctional therapy, nerve stimulation devices, and upper airway surgery offer meaningful paths to airway control depending on apnea severity and individual anatomy.
This article was developed with the clinical expertise of Dr. Avinesh Bhar, Founder at Sliiip.com. Dr. Bhar works with patients across all 50 states via telemedicine and regularly guides patients through the full landscape of sleep apnea treatment options, with particular focus on finding the right fit for each individual’s anatomy, severity, and lifestyle.
If CPAP has not worked for you, you are not alone and you are not out of options. Roughly 30 to 50 percent of patients prescribed CPAP do not use it consistently enough to achieve therapeutic benefit. The reasons vary: mask discomfort, claustrophobia, noise, air pressure intolerance, travel difficulties, and simply not being able to fall asleep while wearing equipment. These are real barriers. They do not mean your sleep apnea cannot be managed.
What follows is an evidence-based overview of the alternatives, organized by evidence strength and typical clinical use case.
Medical Disclaimer: This article is for educational purposes only. Sleep apnea is a medical condition that requires a formal diagnosis and physician-guided treatment. The appropriateness of any alternative to CPAP depends on your AHI severity, anatomy, and health history. This article does not constitute medical advice or a treatment recommendation.
Why CPAP Is Not the Only Answer
CPAP (Continuous Positive Airway Pressure) remains the most widely prescribed treatment for moderate to severe obstructive sleep apnea because it is highly effective when used consistently. It works by delivering a continuous stream of pressurized air through a mask, pneumatically splinting the airway open during sleep.

The problem is not the mechanism. The problem is adherence. A treatment that works in theory but is not used in practice provides no clinical benefit.
The American Academy of Sleep Medicine (AASM) recognizes oral appliance therapy as a first-line treatment alternative precisely because a therapy that is used consistently, even if slightly less effective in controlled conditions, produces better real-world outcomes than a superior therapy that is abandoned.

If you have struggled with CPAP, the first step is understanding why. There are reasons CPAP might not feel like it is working that are correctable with the right adjustments. A physician consultation on why CPAP may not feel effective can sometimes resolve issues before exploring alternatives. But if CPAP is genuinely not a viable path for you, the options below represent evidence-based, clinically recognized alternatives.
Myth vs. Reality: CPAP Alternatives
Myth: If CPAP does not work for you, nothing will.
Reality: The clinical literature includes robust evidence for multiple non-CPAP treatments. Oral appliance therapy, positional therapy, and hypoglossal nerve stimulation each have randomized controlled trial support. Calling them “second-best” misrepresents how treatment matching actually works in practice.
Myth: Alternatives only work for mild sleep apnea.
Reality: Oral appliance therapy is effective for mild to moderate sleep apnea and is considered an acceptable alternative for moderate to severe cases in CPAP-intolerant patients. Hypoglossal nerve stimulation is specifically designed for moderate to severe apnea. The right alternative depends on severity and anatomy, not a one-size categorization.
Myth: Alternatives are harder to access than CPAP.
Reality: Oral appliance therapy is accessible through sleep physicians and dental sleep medicine providers. Home sleep testing followed by a telemedicine consultation can initiate the evaluation process without requiring an in-person clinic visit.
SLIIIP’s board-certified sleep physicians can evaluate the best sleep apnea treatment for you. Virtual consultations in all 50 states. Home sleep tests shipped to your door.
Alternative 1: Oral Appliance Therapy
Oral appliance therapy is the most evidence-supported and most commonly used non-CPAP treatment for obstructive sleep apnea. It is the AASM-endorsed first-line alternative for patients with mild to moderate sleep apnea and for CPAP-intolerant patients with moderate to severe apnea.

A custom-fitted oral appliance, also called a mandibular advancement device (MAD), repositions the lower jaw forward during sleep. This forward positioning keeps the tongue and soft palate from collapsing toward the back of the throat, maintaining airway patency without air pressure or a mask.
The device is worn in the mouth like a mouthguard. It requires no electricity, no machine, and no hose. It fits in a travel case the size of a glasses holder. Most patients who transition from CPAP to oral appliance therapy report significant improvement in comfort and acceptance.

Clinical studies show AHI reductions of 50 percent or more in a majority of mild to moderate sleep apnea patients using a custom-fitted appliance. Patient satisfaction rates with oral appliance therapy consistently exceed those for CPAP in comparative studies, and real-world nightly usage rates are higher.
Not all oral appliances are equivalent. A custom-fitted device fabricated from a dental impression provides significantly better fit, titration capability, and clinical effectiveness than over-the-counter options. Understanding the best oral appliance options for sleep apnea involves assessing jaw anatomy, dental health, and apnea severity. A sleep physician can refer patients to a dental sleep medicine provider for appliance fabrication and fitting.
Expert Q&A with a Sleep Dentist
Q: I think the oral appliance will be uncomfortable.
“Many patients assume that any device used during sleep will be bulky or uncomfortable. What I often find is that most patients in rural settings are not even aware that oral appliances exist as a treatment option for sleep apnea. During screening conversations, I explain that these devices are typically custom-made and much smaller than people expect, and I encourage patients to discuss this option further with qualified sleep physicians and dentists trained in dental sleep medicine.”
Q: Does insurance cover oral appliance?
“Many patients I speak with are not aware that sleep apnea treatment is considered a medical issue. When they ask about insurance coverage for oral appliances used to treat Obstructive Sleep Apnea. I encourage them to discuss this with their physician or sleep clinic after a proper diagnosis, since coverage varies between plans.”
Dr. Anjali
BDS, MDS (Pediatric and Preventive Dentistry)
Post Doc (Restorative Dentistry), UCLA
Dentist at a Rural Health Clinic, California
Alternative 2: Positional Therapy
For patients whose sleep apnea occurs predominantly or exclusively in the supine position, positional therapy is a highly targeted and evidence-supported intervention.
Obstructive sleep apnea is defined as positional when AHI in the supine position is at least twice the AHI in the non-supine position. Research suggests that approximately 50 to 60 percent of patients with obstructive sleep apnea have this positional component. For a subset, AHI in the lateral position falls below the diagnostic threshold entirely.
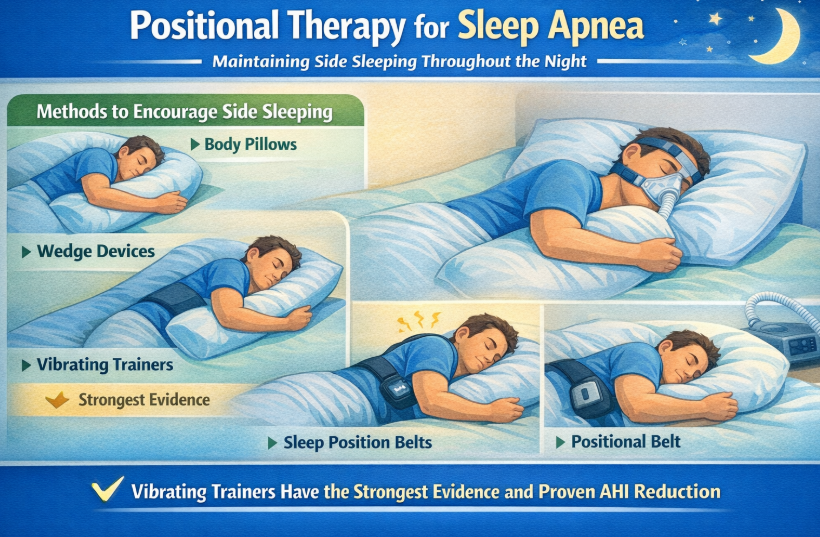
Positional therapy involves maintaining side sleeping throughout the night. Methods include body pillows, wedge devices, vibrating positional trainers that alert the wearer when they roll supine, and purpose-designed sleep position belts. The vibrating trainer approach has the strongest evidence, with multiple randomized trials demonstrating sustained positional compliance and AHI reduction.
Reviewing best sleeping positions for sleep apnea is a practical starting point for understanding this approach.
SLIIIP’s board-certified sleep physicians can evaluate the best sleep apnea treatment for you. Virtual consultations in all 50 states. Home sleep tests shipped to your door.
Alternative 3: Weight Management and Metabolic Intervention
Excess body weight, particularly adipose tissue in the neck and pharyngeal region, is one of the most significant anatomical contributors to airway collapsibility during sleep. For patients with obesity-related sleep apnea, weight reduction is among the most impactful interventions available.
Clinically significant weight loss of five percent or more of body weight is associated with meaningful AHI reduction in most patients with excess weight. Significant weight loss of 10 percent or more has been associated with AHI normalization in some patients with mild to moderate apnea. The relationship between losing weight and reducing sleep apnea is supported by multiple prospective studies.
Weight management is not a standalone solution for most patients with moderate to severe apnea, and it requires time to produce results. But for patients with weight-related apnea, it is one of the most durable long-term interventions available.
Alternative 4: Myofunctional Therapy
Myofunctional therapy involves targeted exercises for the muscles of the tongue, throat, soft palate, and face. The goal is to improve neuromuscular tone in the upper airway so that it is less prone to collapse during sleep.
A systematic review and meta-analysis published in Sleep found that myofunctional therapy reduced AHI by approximately 50 percent in adults and 62 percent in children with obstructive sleep apnea. These are clinically meaningful reductions, particularly for patients with mild to moderate severity.
Myofunctional therapy is typically delivered by a certified orofacial myologist or speech-language pathologist trained in airway function. It requires a commitment to daily exercises over a period of weeks to months. Results are maintained with ongoing practice.
Alternative 5: Hypoglossal Nerve Stimulation
For patients with moderate to severe obstructive sleep apnea who have failed CPAP and meet specific eligibility criteria, hypoglossal nerve stimulation represents a more advanced non-mask treatment option. An implanted device detects breathing patterns and delivers a gentle electrical impulse to the hypoglossal nerve, keeping the tongue and soft palate forward and the airway open.
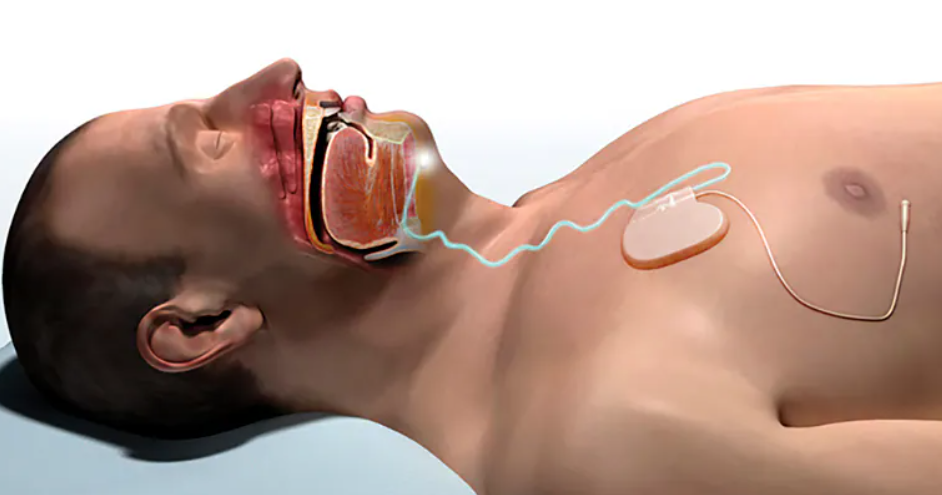
This is a surgical intervention with specific candidacy requirements. Patients must have confirmed moderate to severe obstructive sleep apnea, documented CPAP failure, a BMI generally at or below 32, and a specific airway collapse pattern confirmed by evaluation. The STAR trial published in the New England Journal of Medicine showed a median AHI reduction of approximately 68 percent in appropriately selected patients.
Alternative 6: Upper Airway Surgery
Surgical procedures that modify the anatomy of the upper airway to reduce obstruction have been used for decades as a sleep apnea treatment. The most common procedures target the soft palate, uvula, tonsils, nasal passages, and tongue base.
Uvulopalatopharyngoplasty (UPPP) removes or repositions soft tissue in the throat. Tongue base reduction, genioglossus advancement, and maxillomandibular advancement (MMA) address different structural contributors depending on where the obstruction occurs.
Surgical outcomes vary significantly based on anatomy, procedure selection, and surgeon expertise. MMA, which physically moves the upper and lower jaw forward, shows the strongest evidence for AHI reduction and is considered the most reliably effective surgical option for appropriately selected patients.
Surgery is generally considered after non-surgical options have been exhausted or when anatomical features such as large tonsils, a narrow palate, or jaw structure make surgical correction the most targeted approach. As with any surgical intervention, risks, recovery time, and long-term outcomes should be discussed thoroughly with the surgical team.
Frequently Asked Questions: Sleep Apnea Without CPAP
Can you treat sleep apnea without CPAP? Yes. Multiple evidence-based alternatives exist, including oral appliance therapy, positional therapy, myofunctional therapy, weight management, hypoglossal nerve stimulation, and upper airway surgery. The appropriate option depends on your AHI severity, anatomy, and individual circumstances. A formal diagnosis is the starting point for any treatment decision.
What is the best CPAP alternative for sleep apnea? Oral appliance therapy has the strongest evidence base and is the most widely used CPAP alternative, endorsed by the American Academy of Sleep Medicine as a first-line treatment for mild to moderate sleep apnea and as an appropriate alternative for CPAP-intolerant patients with moderate to severe apnea. Custom-fitted devices from dental sleep medicine providers are significantly more effective than over-the-counter options.
Is oral appliance therapy as effective as CPAP? In controlled conditions, CPAP typically produces greater AHI reduction than oral appliances in patients with severe sleep apnea. In real-world use, however, oral appliance therapy often produces comparable or superior outcomes because patients use it more consistently. A treatment used reliably every night outperforms a more effective treatment used inconsistently.
Can I use an oral appliance for moderate sleep apnea? Yes. The AASM guidelines recognize oral appliance therapy as clinically appropriate for patients with mild to moderate sleep apnea as a primary treatment, and for CPAP-intolerant patients with moderate to severe apnea as an alternative. Follow-up testing after starting oral appliance therapy confirms whether your AHI is adequately controlled.
Does positional therapy work for sleep apnea? For patients with positional sleep apnea, where AHI in the back-sleeping position is significantly higher than in the side-sleeping position, positional therapy can be highly effective. Studies show AHI reductions of 30 to 50 percent or more in positional sleep apnea patients who maintain consistent side sleeping.
Can weight loss cure sleep apnea? In some patients with mild obesity-related sleep apnea, significant weight loss has been associated with AHI normalization. For most patients with moderate to severe sleep apnea, weight loss reduces severity meaningfully but does not eliminate the condition on its own. It works best as part of a comprehensive treatment approach.
What is myofunctional therapy for sleep apnea? Myofunctional therapy is a structured program of exercises for the tongue, throat, and facial muscles that improves upper airway muscle tone. Clinical research shows AHI reductions of approximately 50 percent in adults who complete a full course. It is most effective as a complement to other treatments such as oral appliance therapy.
Is surgery an option for sleep apnea without CPAP? Yes. Several upper airway surgical procedures are available for appropriate candidates. Maxillomandibular advancement (MMA) has the strongest evidence for significant AHI reduction. Surgical options are generally considered after non-surgical alternatives have been evaluated, and outcomes depend heavily on anatomy and patient selection.
What is hypoglossal nerve stimulation? Hypoglossal nerve stimulation is a surgically implanted device that monitors breathing and delivers gentle electrical pulses to the hypoglossal nerve during sleep, keeping the tongue and airway open. It is designed for moderate to severe sleep apnea patients who have failed CPAP and meet specific candidacy criteria. Clinical trials show median AHI reductions of approximately 68 percent in appropriate candidates.
How do I know which CPAP alternative is right for me? The appropriate alternative depends on your AHI severity, airway anatomy, and personal circumstances. A formal sleep study provides your AHI score, which is the foundation of any treatment decision. A board-certified sleep physician can then evaluate which options are clinically appropriate for your specific profile.
Can I use a mouthguard from a pharmacy for sleep apnea? Over-the-counter mouthguards are not equivalent to custom-fitted oral appliances from a dental sleep medicine provider. They do not offer the same level of mandibular advancement precision, comfort, or titration capability. Clinical evidence for sleep apnea treatment is based on custom-fitted devices. A store-bought guard may reduce snoring but is unlikely to provide adequate AHI control for documented sleep apnea.
Does insurance cover sleep apnea alternatives to CPAP? Many insurance plans cover oral appliance therapy when prescribed by a sleep physician and fabricated by a qualified dental provider, particularly when CPAP intolerance is documented. Coverage varies by plan. A sleep physician evaluation and a verified home sleep test diagnosis are typically required to initiate insurance authorization for any treatment.
Latest posts
-
Digital Sunset: Build a Low-Tech Bedroom for Sleep
A digital sunset, the simple habit of powering down screens and dimming light well before bed, is a routine Dr. Avinesh Bhar, Board-Certified Sleep Physician at SLIIIP.com, often suggests to…
-
Scandinavian Sleep Method: Two Duvets, Better Rest
The Scandinavian sleep method, the Nordic habit of sharing a bed while using two separate duvets instead of one, is an idea Dr. Avinesh Bhar, Board-Certified Sleep Physician at SLIIIP.com,…
-
Sleep Tourism: Can a Rest Vacation Actually Reset Your Sleep?
Sleep tourism, the growing trend of booking trips built entirely around better rest, is something Dr. Avinesh Bhar, Board-Certified Sleep Physician at SLIIIP.com, sees more travelers curious about as hotels…
Get updates
Spam-free subscription, we guarantee. This is just a friendly ping when new content is out.

