👉 Register for Free. How to Diagnose Sleep Apnea Faster in Primary Care – FREE Webinar by Dr. Audrey Wells. – Friday, April 24 at 12 PM ET


Central vs Obstructive Sleep Apnea: Key Differences, Symptoms, and What to Know
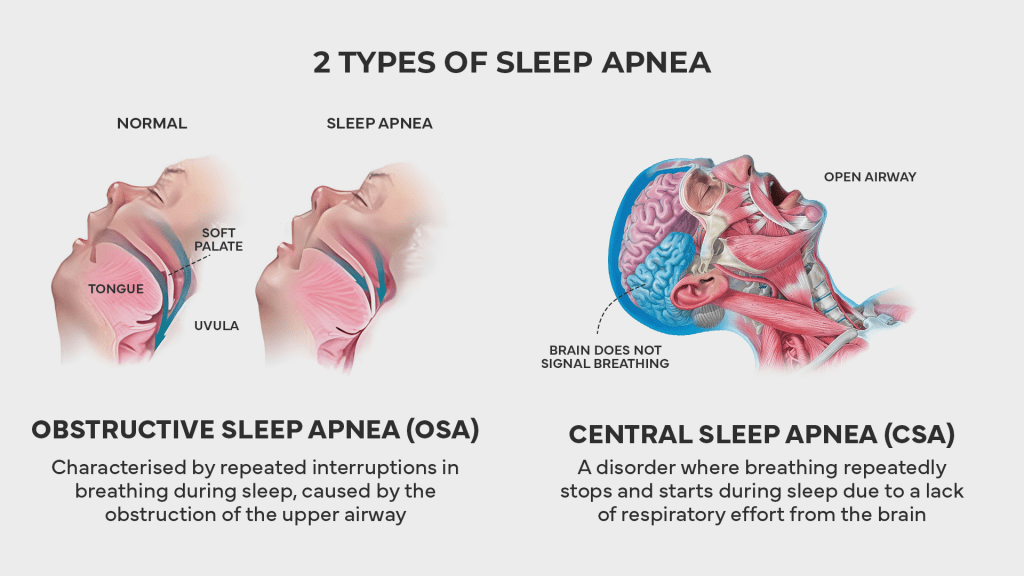
When most people hear the term “sleep apnea,” they picture a single condition. But sleep apnea is not one-size-fits-all. There are two distinct types which are central vs obstructive sleep apnea.
Dr. Avinesh Bhar, the Founder of SLIIIP, is also a sleep apnea sufferer. He has helped thousands get properly evaluated and find the right care for their specific type of sleep apnea, and he and his team of board-certified sleep medicine physicians can help you too. This guide breaks down everything you need to know about central vs obstructive sleep apnea so you can understand the key differences and what they mean for you.
Obstructive Sleep Apnea: A Physical Blockage
Obstructive sleep apnea, commonly abbreviated as OSA, is the more prevalent of the two types. It is estimated to affect up to 30 percent of adults, though the majority of those individuals remain unaware of their condition. OSA occurs when the muscles in the throat and the base of the tongue relax during sleep. When those muscles lose their tension, the surrounding soft tissue can collapse inward and partially or completely block the upper airway.
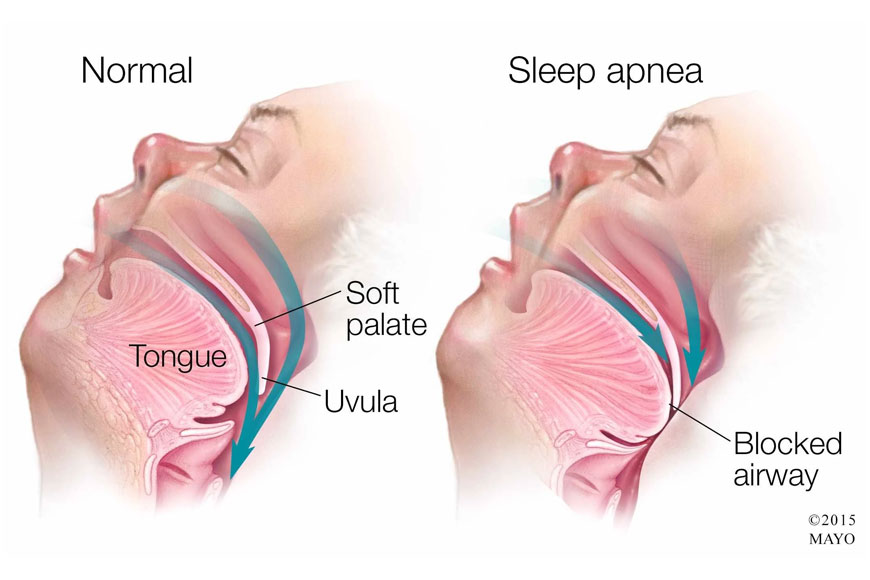
The hallmark symptom of obstructive sleep apnea is loud snoring. As air squeezes past the partially collapsed tissue, it creates vibration, which produces the familiar sound. Gasping, choking, or snorting sounds are also common, particularly during the moments when breathing resumes after a pause. SLIIIP has a detailed exploration of the signs of sleep apnea that can help you recognize whether these patterns are present in your own experience.
Other common indicators include excessive daytime sleepiness, morning headaches, a dry mouth upon waking, difficulty concentrating, and mood changes. Because these symptoms develop gradually and can be attributed to other causes, many people live with OSA for years before it is identified. If you have experienced the frustrating pattern of sleeping a full night yet waking up tired, obstructive sleep apnea is one of the conditions worth exploring.
Book a Sleep Evaluation With Our Board-Certified Sleep Doctors
SLIIIP’s team of board-certified sleep medicine physicians is licensed in 40 states and experienced in evaluating both obstructive and central sleep apnea. No referral needed. No long waits. Consultations happen from the comfort of your home via telemedicine.
We can help with: Obstructive Sleep Apnea, Central Sleep Apnea, Complex Sleep Apnea, Home Sleep Testing, CPAP and BiPAP Therapy, Oral Appliance Therapy, Snoring, Chronic Fatigue and Daytime Sleepiness, Sleep-Related Breathing Disorders.
We accept Medicare, Tricare, and most major insurance plans. Book your appointment today.
Central Sleep Apnea: A Brain Signaling Issue
Central sleep apnea, or CSA, is far less common than its obstructive counterpart. Fewer than one percent of adults are estimated to have this type. Unlike OSA, there is no physical blockage of the airway. Instead, the issue lies in the brain’s signaling system. During episodes of central sleep apnea, the brain temporarily fails to send the appropriate signals to the muscles responsible for breathing. The airway remains open, but the body simply does not make the effort to inhale.
When this happens, oxygen levels in the blood begin to drop and carbon dioxide levels begin to rise. Eventually, the imbalance triggers the brain to restart breathing, often with a sudden gasp or a jolt that briefly wakes the person. Like OSA, these awakenings are usually too brief to be remembered, but they fragment sleep and prevent the body from getting the rest it needs.
Central sleep apnea is frequently associated with other underlying health conditions. Heart failure is one of the most common, along with stroke, kidney failure, and certain neurological conditions that affect the brainstem. Long-term use of opioid medications can also disrupt the brain’s respiratory control center and contribute to the development of CSA. The connection between sleep apnea and cardiovascular health is particularly relevant for those with central sleep apnea, as the two conditions are often closely intertwined.
The Core Difference: Blockage vs Signal
The simplest way to understand the distinction is through analogy. Think of obstructive sleep apnea as a clogged pipe. The pump is working, your body is trying to breathe, but the airway is physically blocked by collapsed tissue. You can see evidence of this effort in the movement of the chest and abdomen, which may appear to be working against each other as the body tries to push air past the obstruction.
Here is an example of breathing sounds in a sleep apnea sufferer. Check your breathing sounds
tonight and that of your partners.
Central sleep apnea is more like a power outage. The pipe is clear and there is nothing physically blocking the airway, but the pump has temporarily stopped running because the brain failed to send the signal to keep it going. During a central event, there is no chest or abdominal movement at all, because the body is simply not attempting to breathe.
This mechanical difference is important for several reasons. It affects how the condition is detected during a sleep study, how it is classified by severity, and which management approaches are most likely to be effective.
Symptom Overlap and Key Differences
Both types of sleep apnea share several symptoms, which can make distinguishing between them challenging without a formal evaluation. Daytime sleepiness, fatigue, difficulty concentrating, and mood changes are common to both. Both can cause disrupted sleep and leave you feeling unrefreshed in the morning. The experience of brain fog is another symptom that can appear with either type.

However, there are some notable differences. Loud, chronic snoring is much more strongly associated with obstructive sleep apnea. People with central sleep apnea may snore, but it tends to be less prominent. CSA is also more likely to present with shortness of breath upon waking, and the condition is more commonly found in people with existing cardiac or neurological conditions.
Another important difference is the pattern of breathing events. In obstructive sleep apnea, the events tend to occur more randomly throughout the night. In certain types of central sleep apnea, particularly Cheyne-Stokes breathing, there is a recognizable pattern of gradually increasing and then decreasing breathing effort, followed by a pause. This pattern is most commonly seen in people with heart failure.
Complex Sleep Apnea: When Both Types Coexist
There is a third category worth understanding. Complex sleep apnea, also called treatment-emergent central sleep apnea, occurs when someone who has been identified with obstructive sleep apnea begins using CPAP therapy, and central apnea events emerge during the process. In other words, once the obstructive component is resolved by keeping the airway open with pressurized air, the brain’s signaling irregularities become apparent.
Complex sleep apnea affects a relatively small percentage of people, estimated at around 2 to 3 percent of the general population. It often requires a different type of positive airway pressure device, such as adaptive servo-ventilation (ASV), which adjusts the air pressure in response to the person’s breathing patterns rather than delivering a constant stream.
For a broader understanding of the condition and its categories, SLIIIP’s comprehensive overview of sleep apnea covers the full picture.
Not Sure Which Type of Sleep Apnea You Have?
SLIIIP’s board-certified sleep medicine physicians are licensed in 40 states and specialize in identifying and managing all types of sleep apnea. Get evaluated from home with no referral required.
We can help with: Obstructive Sleep Apnea Evaluation, Central Sleep Apnea Evaluation, Complex Sleep Apnea, Home Sleep Testing, CPAP and BiPAP Therapy, Oral Appliance Therapy, Snoring Assessment, Excessive Daytime Sleepiness.
We accept Medicare, Tricare, and most major insurance plans. Schedule your evaluation now.
What Causes Each Type
The risk factors for obstructive and central sleep apnea are quite different, reflecting their different underlying mechanisms.
For obstructive sleep apnea, the primary risk factors are structural and lifestyle-related. Excess body weight is one of the most significant, as fat deposits around the neck can compress the airway. Other factors include a naturally narrow airway, enlarged tonsils or adenoids, a large tongue, a thick neck circumference, and a receding jaw. SLIIIP has explored the role of weight in the development of sleep apnea in detail.
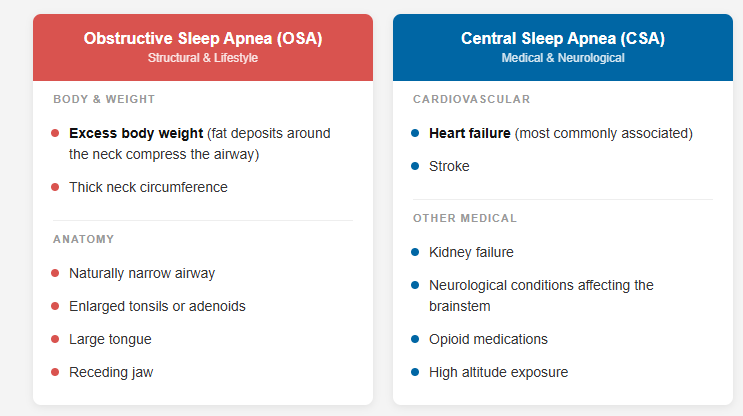
For central sleep apnea, the risk factors tend to be medical in nature. Heart failure is the most commonly associated condition, followed by stroke, kidney failure, and neurological conditions affecting the brainstem. Opioid medications are a recognized contributor. High altitude can also trigger central apnea events in some individuals. Like OSA, central sleep apnea is more common in men and in older adults.
How Each Type Is Identified
Both types of sleep apnea are identified through a sleep study, or polysomnography. However, the studies look at different signals to distinguish between the two. During a sleep study, sensors monitor your airflow, chest and abdominal movement, blood oxygen levels, brain activity, and heart rate.

Home sleep tests, which are an increasingly popular and convenient option for initial evaluation, are generally best suited for identifying obstructive sleep apnea. They can detect central events in some cases, but a full in-lab polysomnography may be recommended if central sleep apnea is suspected. If you are considering the first step toward evaluation, SLIIIP’s guide on home sleep apnea testing provides a clear overview of how the process works, and you can explore the differences between home and lab sleep tests to determine which option may be right for you.
Management Approaches for Each Type
Because the two types have different causes, they require different management strategies. For obstructive sleep apnea, the most commonly used approach is CPAP therapy, which delivers a continuous stream of pressurized air through a mask to keep the airway open during sleep. CPAP is highly effective when used consistently. For those who find CPAP difficult to tolerate, oral appliances that reposition the jaw forward offer an alternative, particularly for mild to moderate cases. SLIIIP provides a review of the top-rated oral appliances for those exploring this option.

Lifestyle changes also play an important role in managing OSA. Maintaining a healthy weight, reducing alcohol consumption, avoiding sedatives before bed, and adjusting sleep position can all contribute to fewer breathing disruptions. SLIIIP has looked at how weight management can help reduce sleep apnea for those interested in this approach.
For central sleep apnea, management often begins with addressing the underlying condition. If heart failure is the primary driver, optimizing cardiac care may help reduce central apnea events. If opioid medications are contributing, a medication review with a healthcare provider is an important step.
In terms of device-based management, standard CPAP is sometimes effective for CSA, but more specialized options are often needed. Bilevel positive airway pressure (BiPAP) provides different pressure levels for inhalation and exhalation. Adaptive servo-ventilation (ASV) is a more advanced option that automatically adjusts pressure in response to the person’s breathing patterns. These devices are typically prescribed and calibrated by a sleep specialist based on the individual’s specific needs.
Why the Distinction Matters
Understanding whether you have obstructive or central sleep apnea is not an academic exercise. It directly affects which approach is likely to work for you. Using CPAP therapy that is calibrated for OSA may not adequately address central events, and in some cases, it can even make them worse. Conversely, the lifestyle modifications that are highly effective for OSA may have limited impact on CSA if the underlying cause is neurological or cardiac in nature.
A proper evaluation through a sleep study is the only reliable way to determine which type you have. If you are unsure whether your symptoms warrant further investigation, SLIIIP’s sleep apnea quiz is a helpful starting point. And for those ready to take the next step, getting a home sleep test through SLIIIP is a straightforward process that can provide the data you and your healthcare provider need to move forward. At SLIIIP we work with these health insurances and can work with your insurance to get your sleep treatment approved.

Frequently Asked Questions About Central vs Obstructive Sleep Apnea
What is the main difference between central and obstructive sleep apnea?
Obstructive sleep apnea is caused by a physical blockage of the airway when throat muscles relax during sleep. Central sleep apnea occurs when the brain fails to send the proper signals to the muscles that control breathing. The airway may remain open during central events.
Which type of sleep apnea is more common?
Obstructive sleep apnea is far more common, affecting up to 30 percent of adults. Central sleep apnea affects fewer than one percent of the adult population.
Can you have both types at the same time?
Yes. This is called complex or mixed sleep apnea. It can also develop as treatment-emergent central sleep apnea when CPAP therapy for OSA reveals underlying central apnea events.
Does central sleep apnea cause snoring?
Central sleep apnea may involve some snoring, but it is typically less prominent than in obstructive sleep apnea. Loud, chronic snoring is more strongly associated with OSA.
Is central sleep apnea more dangerous than obstructive?
Both types carry health considerations. Some research suggests central sleep apnea may be associated with a higher risk of certain complications, partly because it is often linked to serious underlying conditions like heart failure. However, both types benefit from appropriate management.
What conditions are associated with central sleep apnea?
Heart failure is the most common association, followed by stroke, kidney failure, neurological conditions affecting the brainstem, and long-term opioid medication use.
Can CPAP work for central sleep apnea?
Standard CPAP can help some people with CSA, but more specialized devices like BiPAP or adaptive servo-ventilation (ASV) are often more effective because they adjust to the person’s breathing patterns.
How is the type of sleep apnea determined?
A sleep study (polysomnography) monitors both airflow and respiratory effort. In OSA, effort continues during airflow pauses. In CSA, both airflow and effort stop simultaneously.
Can lifestyle changes help central sleep apnea?
Lifestyle changes like reducing alcohol and maintaining a healthy weight may provide some benefit, but CSA management primarily focuses on addressing the underlying medical condition and using appropriate positive airway pressure devices.
Is central sleep apnea hereditary?
There is some evidence that genetic factors can influence the brain’s respiratory control system, but CSA is more commonly linked to acquired conditions like heart failure or medication use rather than inherited traits.
Can obstructive sleep apnea turn into central sleep apnea?
Not exactly, but treatment-emergent central sleep apnea can develop when CPAP therapy resolves the obstructive component, revealing underlying central events that were previously masked.
Do home sleep tests detect central sleep apnea?
Home sleep tests are primarily designed to detect obstructive sleep apnea. While they may capture some central events, a full in-lab polysomnography is generally recommended if central sleep apnea is suspected.
Is one type of sleep apnea easier to manage?
Obstructive sleep apnea generally has more management options and responds well to widely available approaches like CPAP and oral appliances. Central sleep apnea can be more challenging because it often involves managing underlying medical conditions.
Can children have central sleep apnea?
Yes, though it is rare. Premature infants are more susceptible to central apnea events. In older children, central sleep apnea is usually associated with an underlying neurological or cardiac condition.
What is Cheyne-Stokes breathing?
Cheyne-Stokes breathing is a specific pattern associated with central sleep apnea, most commonly seen in people with heart failure. It involves a gradual increase and then decrease in breathing effort, followed by a pause, in a repetitive cycle.
Can medications cause central sleep apnea?
Yes. Opioid medications are the most commonly recognized pharmaceutical contributor to central sleep apnea. They can disrupt the brain’s ability to regulate breathing during sleep.
Does sleeping on your side help central sleep apnea?
Positional changes are more beneficial for obstructive sleep apnea. Because CSA is a brain signaling issue rather than a physical obstruction, sleep position typically has less impact on central events.
What does complex sleep apnea mean for my management?
Complex sleep apnea usually requires a device that can address both obstructive and central events. Adaptive servo-ventilation (ASV) is often the preferred approach, as it dynamically adjusts to the person’s breathing patterns.
Can central sleep apnea improve on its own?
In some cases, if the underlying cause is addressed, such as effective heart failure management or discontinuation of contributing medications, central sleep apnea events may decrease. However, ongoing monitoring is important.
Should I see a specialist if I suspect I have sleep apnea?
Yes. A sleep specialist can determine which type of sleep apnea you have through a proper sleep study and recommend the most appropriate management approach for your specific situation.
Latest posts
-
Beyond the CPAP: What a Comprehensive Sleep Care Plan Actually Looks Like
A good sleep care plan goes far beyond a single machine, and Dr. Avinesh Bhar, Board-Certified Sleep Physician at SLIIIP.com, explains that real, lasting results come from a personalized approach,…
-
The Cortisol Switch: Why You Feel Exhausted All Day But “Wired” at Bedtime
Cortisol follows a natural daily rhythm that helps you feel alert in the morning and calm at night, and Dr. Avinesh Bhar, Board-Certified Sleep Physician at SLIIIP.com, explains that when…
-
Can You Use an Oral Appliance with Dentures or Missing Teeth
An oral appliance is a popular option for snoring and sleep apnea, and Dr. Avinesh Bhar, Board-Certified Sleep Physician at SLIIIP.com, explains that whether one can work with dentures or…
Get updates
Spam-free subscription, we guarantee. This is just a friendly ping when new content is out.

